Introduction
Osteoma of the temporal bone is benign pedunculated tumors of the lamellar bone that are most commonly found in the external auditory canal. Osteomas in the middle ear are not common, and since their first mention,1) only 25 relevant cases (18 papers) have been reported in the literature. In previously reported cases, osteomas in the middle ear were combined with cholesteatoma or ossicular osteoma. However, osteoma of the promontory of the middle ear is even rarer, with only 5 cases reported to date.2,3,4,5,6) This study reports a case of asymptomatic osteoma of the promontory in the middle ear mimicking a congenital cholesteatoma in a 4-year-old girl.
Case Report
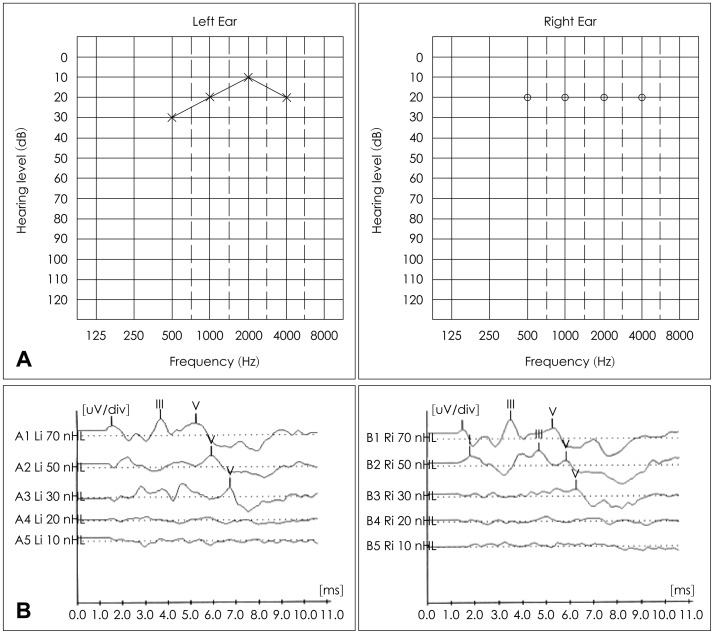
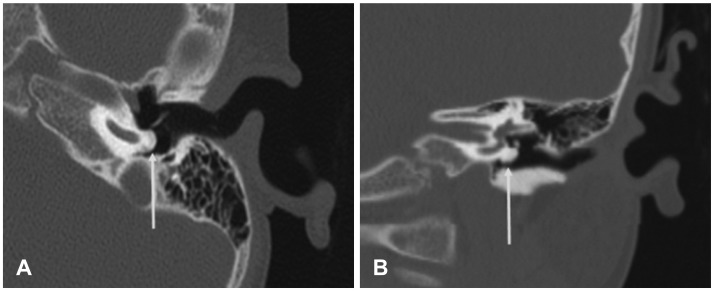
The patient whose case is presented here was a 4-year-old girl without a history of hearing loss and otorrhea. She denied dizziness and tinnitus. Having been diagnosed with congenital cholesteatoma at a local clinic, she was transferred to our department. Otoendoscopic examination revealed a white mass behind the left tympanic membrane mimicking a congenital cholesteatoma (Fig. 1). A MASTER (Bio-logic, San Carlos, CA, USA) system was used for auditory steady-state response, auditory brainstem response measurement. It revealed normal range of hearing (Fig. 2). Temporal bone high resolution computerized tomography was conducted with Discovery CT 750 (GE, New York, NY, USA). Slice thickness is 1.25 mm and it disclosed the presence of bony mass covering the left cochlear promontory at the level of the basal turn (Fig. 3). In radiological examination, this mass was identified as an osteoma. The bony mass did not involve the ossicles, oval and round windows, or obstruction of the Eustachian tube orifice. No further anomalies were observed. This asymptomatic mass was not removed. Periodical follow-up with temporal bone high resolution computed tomography was needed.
Discussion
Osteoma of the temporal bone most commonly occurs in the external ear. On rare occasions, it may arise from other locations within the temporal bone, such as the ossicle (malleus, incus), lateral semicircular canal7) and the petrous ridge.8)
Osteomas on ossicle may cause a conductive hearing loss by impinging on the ossicular chain. However there is no related sensorineural hearing loss.9,10,11,12)
The etiology of the osteoma of the promontory remains unknown. Most of the cases of middle-ear osteomas were asymptomatic and were diagnosed coincidentally. In the present case, the osteoma was asymptomatic. Hearing tests revealed the normal range. If the patient has a conductive hearing loss, surgical intervention can be performed using exploratory tympanotomy. Care should be taken not to avoid damage to the ossicular chain or iatrogenic labyrinthine fistula. In Cremers,2) the promontory osteoma was removed using a chisel, but the traumatic labyrinthine fistula was followed. If the mass is asymptomatic or when it does not involve the ossicular chain, surgical removal is not necessary. Periodical follow-up with HRCT and audiologic examination is needed. In case of progressive growth of the osteoma with an increasing hearing loss, ossicular chain involvement, obstruction of Eustachian tube, or round window obstruction, surgery should be considered.