Better Understanding of Direct Bone-Conduction Measurement: Comparison with Frequency-Specific Bone-Conduction Tones and Brainstem Responses
Article information

Abstract
Background and Objectives
The present study aimed to compare thresholds of direct bone-conduction (BC direct) with those of behaviorally measured BC pure-tone audiometry (PTA) and objectively measured BC auditory brainstem response (ABR) to confirm the clinical feasibility of their relationships.
Subjects and Methods
Young adults with normal hearing participated in the study to determine the thresholds from three measurements at four testing frequencies. In the BC direct, the vibrator of a bone-anchored hearing aid softband was placed on the right mastoid of each subject. In both PTA and ABR, a B71 bone oscillator was placed on the subject’s right mastoid. While the subject’s thresholds of BC direct and BC PTA were determined with a clinically routine 5-dB step procedure, BC ABR was conducted to determine the individual’s hearing sensitivity by a peak V of the waveform using tone-burst and click stimuli.
Results
The BC direct showed a different pattern between low and high frequencies. Precisely, its thresholds were 13.25 and 12.25 dB HL at 0.5 and 1 kHz, respectively, but 19 and 19.75 dB HL at 2 and 4 kHz, respectively. A significant positive correlation existed between BC direct and PTA at 1 kHz, which was also correlated with ABR.
Conclusions
Based on the current data, the thresholds of BC direct were similar to BC PTA at low frequencies and BC ABR at high frequencies. The thresholds of BC direct might be predictable at approximately 5 dB higher (or lower) than that in PTA, although a large data set is required for standardization.
Introduction
It is generally acknowledged that single-sided deafness, a profound sensorineural hearing loss in one ear with normal hearing in the other, can be treated with bone-anchored hearing systems (BAHSs) in the clinic [1]. Some patients with conductive or mixed hearing loss may also benefit from BAHSs, particularly those who have unilateral and/or bilateral hearing loss of at the most 50-60 dB HL and correct responses of ≥60% in speech recognition [2].
Currently, BAHSs have provided technical advantages to many patients in terms of better hygiene control and cosmetic concerns. For example, House and Kutz [3] suggested a new attachment technique via an external magnet rather than percutaneous abutment via a titanium screw, which increased the patient’s risk of possible infection or skin overgrowth. Jang, et al. [4] confirmed the utility of a simple surgical procedure with a small incision and no risk of inner ear damage. Such technical advantages might provide a high satisfaction rate for users. Consequently, Flynn, et al. [5], who measured thresholds of patients with mixed hearing loss with BAHS implants, showed that the aided thresholds in patients were within the audible range for speech, indicating that BAHSs can offer as much significant benefit as conventional air-conduction hearing aids in terms of audibility and sound quality. While reporting a similar amount of threshold benefits as those by Flynn, et al., [5] Ricci, et al. [6] additionally confirmed improved scores in speech discrimination in patients with conductive and mixed hearing loss with BAHS implants.
Nevertheless, since the amount of amplification provided by the BAHS is based on the individual’s frequency-specific sensorineural thresholds, reliable results (i.e., thresholds) from clinically objective measurements are necessary to initiate successful fitting for patients with BAHS implants. In detail, for the fitting procedure, clinicians need to determine the air-conduction and bone-conduction (BC) thresholds from the individual’s audiogram. Then, unlike conventional hearing aids that are stimulated by air conduction, they should behaviorally measure direct BC (BC direct) using a software developed by the manufacturer to identify the best fit range. The measurement of BC direct includes sound attenuation through the skin and bone and needs to be considered for appropriate BAHS fitting. Precisely, the BC direct refers to a process of generation and transmission of signals that stem from the BAHS and thus allows direct measurement of the patient’s hearing thresholds through a sound processor. If the amount of sound attenuation is not considered, the gain of the BAHS would be inadequate. Thus, the reliable thresholds obtained by BC direct measurement can support the accuracy of the initial BAHS fitting [7]. Moreover, it may be difficult to fit patients who have passive response, such as young children and/or older adults. As a solution to this problem, Rahne, et al. attempted objective measurements, such as auditory brainstem response (ABR) and cortical auditory evoked potentials (CAEP) in both individuals with normal hearing [8] and those with hearing impairment [9]. Their results suggested that CAEP measurement was the most objective and reliable tool to evaluate the BAHS fitting condition. However, a close look at their studies reveals that they had N1-P1-N2 responses only at 1 and 2 kHz and included large inter- and intra-variance across the subjects (even in normal hearing). In addition to these limitations, cortical responses needed partial cooperation from the patients who were required to be awake during the measurement.
In contrast, pure-tone audiometry (PTA) is popularly used by clinicians because it is convenient and accurate and provides a comprehensive interpretation, while an ABR is an objective tool to confirm an individual’s hearing condition and diagnose otoneural pathology. Both BC PTA and BC ABR have technical limitations in clinical application based on the maximum effective intensity level of approximately 40 dB HL for BC stimuli. Furthermore, an appropriate amount of contralateral masking and high stimulus artifact as a result of electromagnetic energy from the bone vibrator during the measurement need to be considered [10]. However, several clinicians agree that the two measurements are important indicators in understanding cochlear sensitivity [11] and evaluating whether cochlea function is reserved. The present study aimed to compare the thresholds of BC direct with those of behaviorally measured BC PTA and objectively measured BC ABR, to which clinicians are fairly accustomed, and confirm the clinical feasibility of their relationships. The results will help clinicians understand BC direct measurement and determine the differences of the three BC measurements, even though they share the same auditory route, and will be a basis of BAHA fitting even in patients who do not provide an active psychometric response and thus have a difficulty in initiating BAHA fitting.
Subjects and Methods
Participants
Twenty young adults (10 male and 10 female) with normal hearing voluntarily participated in the study. The age ranged from 18 to 24 years [mean, 20.9 years; standard deviation (SD), 1.86]. All participants reported no history of head and neck abnormalities, ear surgery, otologic disease, and head trauma. They also underwent screening tests for participation in this study with a type-A tympanogram, thresholds of ≥15 dB HL in each ear from 0.25 to 8 kHz, and air-bone gaps <5 dB HL. The experimental procedure was approved by the Institutional Review Board of Hallym University (HIRB-2019-025). The participants provided written informed consent before initiation of the study.
Experimental equipment and test stimuli
In the BC direct measurement, the BAHA Fitting Software (version 5.3, Cochlear Ltd., Sydney, Australia) combined with the BAHA® 5 Sound Processor (Cochlear Bone Anchored Solutions AB, Gothenburg, Sweden) was used. The stimuli were presented by a tone of 0.5, 1, 2, and 4 kHz, which is a typical procedure to measure the thresholds in patients with BAHS implants [12]. The thresholds of BC PTA were behaviorally obtained using a B71 bone transducer headset (RadioEar, Middelfart, Denmark) connected to a GSI 61 audiometer (Grason-Stadler Inc., Eden Prairie, MN, USA) while being presented the same frequencies as those in BC direct.
Objectively, BC ABR was recorded with a Bio-logic Navigator Pro (Natus, Pleasanton, CA, USA). Its stimuli were presented using the same bone transducer as that in BC PTA (i.e., RadioEar B71 oscillator) as click and tone burst. In detail, the click stimuli with 100 ms in duration were presented at a rate of 11.1/s with alternating polarity. The tone-burst stimuli were presented at 0.5, 1, 2, and 4 kHz with alternating polarity. They were Blackman gated with two cycles-rise and fall times- and no plateau at a rate of 27.7/s; consequently, the tone-burst stimuli at 0.5, 1, 2, and 4 kHz had a 1.5, 2.0, 3.0, and 4.0 ms rise/fall time, respectively. For the time windows, 16 ms and 21.3 ms were applied for the click and tone-burst stimuli, respectively. Two stimuli were recorded using filter setting of 0.03 to 3 kHz (5 dB/octave) and amplified using a gain of 100,000. The samples >23.8 μV were rejected automatically. However, the maximum levels of stimuli differed depending on the type of stimuli and test frequencies due to high artifact: 50, 60, 70, and 70 dB HL for 0.5, 1, 2, and 4 kHz tone-burst and click stimuli, respectively. At each presentation level, 2,000 sweeps were averaged as minimum.
Experimental procedures and conditions
After conducting the hearing screening, the BC direct was measured in a quiet room. The vibrator of BAHA® 5 softband (Cochlear Bone Anchored Solutions AB) was placed on the right mastoid of each subject to estimate the thresholds. When the signals were generated to the BAHA, the cochlea and/or osseo-integrated implant directly received the signal. The BC direct generated an amplified electromagnetic signal in response to sounds received from the sound processor. The amplified signal was transmitted to the internal device of the participant, and thus the signal caused the magnet to vibrate. Eventually, the vibrations were transmitted to the cochlea where the sounds became recognized [13]. While presenting 50 dB HL as an initial intensity level at each test frequency, the modified method of limits (also called the adaptive method of behavioral thresholds) using 5-dB step was applied to determine its thresholds [14].
Then, BC PTA was performed in a soundproof booth; the bone transducer was placed on the right mastoid of each subject to estimate the thresholds using the standard 5-dB adaptive method. During the BC ABR recording, the same bone vibrator was placed on the right mastoid. Click and tone-burst stimuli were employed using a two-channel ipsilateral electrode montage with Fpz (ground), Fz (active), and left/right ear lobe (reference). Electrode impedance in any pair of electrodes was maintained <5 kΩ. The data were rejected when artifacts exceeded 10% of the total sweep numbers. The stimuli intensity level was initially set to 50-70 dB HL, depending on the test frequency, and then reduced in 5-dB steps until the individual threshold was confirmed. While labeling the wave V peak in the waveform, the thresholds were determined by two audiologists who had considerable experience in ABR recordings.
Statistical analysis
The statistical analysis was performed using two-way analysis of variance (ANOVA) with repeated measurement and Pearson correlation with SPSS software (version 21, IBM Corp., Armonk, NY, USA). In the ANOVA, the independent variables were the three measurements and their test frequencies, and the dependent variables were their thresholds. Pearson correlation was used to analyze any relationship among the thresholds of the three measurements. The criterion used for statistical significance was a p-value<0.05.
Results
Fig. 1 indicates the thresholds of BC PTA, BC direct, and BC ABR in testing frequencies of 0.5, 1, 2, and 4 kHz. Among the measurements, BC PTA showed the lowest thresholds across the frequencies whereas BC ABR had the highest thresholds. For example, four-frequency averages of the PTA and ABR thresholds were 3.81 dB HL (SD, 6.43) and 32.12 dBnHL (SD, 13.99), respectively. However, BC direct provided a different pattern depending on the test frequency: lower thresholds for the low frequencies such as 500 and 1,000 Hz and higher thresholds for 2,000 and 4,000 Hz.
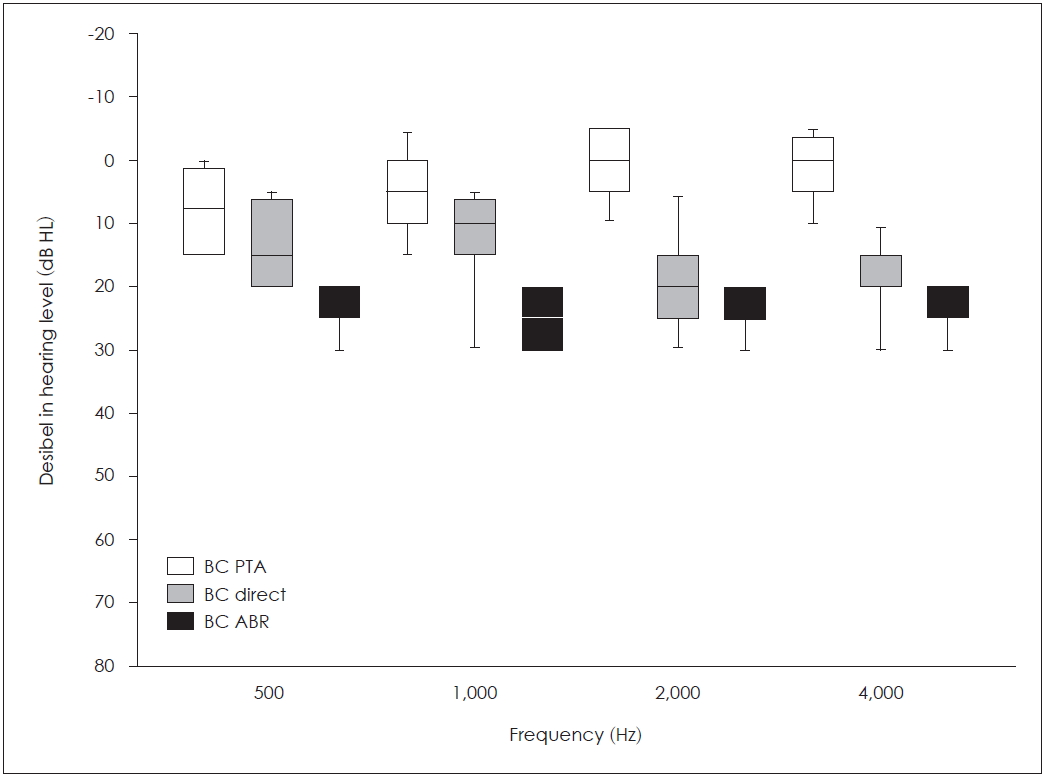
Comparison of bone-conduction (BC) thresholds among three measurements, pure-tone audiometry (PTA), BC direct, and auditory brainstem response (ABR), stimulated by frequency-specific tones at 0.5, 1, 2, and 4 kHz. Noticeably, thresholds of the BC direct were closely located in BC ABR for 2 and 4 kHz.
Based on the results of the ANOVA with repeated measurements, we confirmed a significant difference among the three measurements [F (2, 38)=90.404, p<0.001]. A Bonferroni post hoc test showed that the thresholds of BC PTA (mean, 3.81; SD, 1.01) were significantly lower than those of BC direct (mean, 16.37; SD, 1.27) (p<0.001), which were significantly higher than those of BC ABR (mean, 32.12; SD, 2.11) (p<0.001). However, there was no significant difference in thresholds among the test frequencies [F (3, 57)=0.818, p=0.489]. The interaction between the three measurements and four test frequencies was revealed statistically [F (6, 114)= 5.422, p<0.001] because the thresholds of BC PTA were lower (or better) and BC direct results were increased (or worse) as the test frequency increased.
Interestingly, in the results of pairwise correlation among the three measurements and four test frequencies, a significantly positive correlation existed between BC PTA and BC direct (r=0.515, p=0.020) and between BC PTA and BC ABR at 1 kHz (r=0.445, p=0.049) (Table 1). In more detail, we observed the individual’s threshold of PTA for all subjects as a function of the BC direct thresholds (Fig. 2A) and that of ABR as a function of the PTA thresholds (Fig. 2B).

Pairwise correlations between bone-conduction thresholds of three measurements in four test frequencies
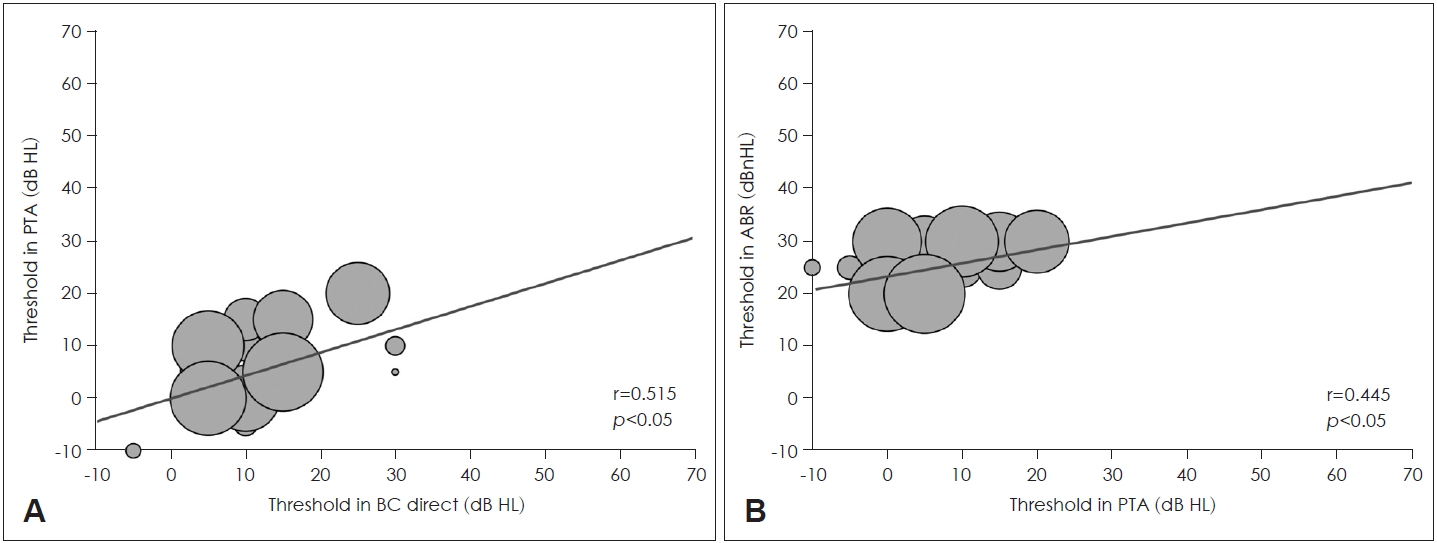
Correlation graphs of an individual’s threshold between pure-tone audiometry (PTA) and bone-conduction (BC) direct (A) and between PTA and auditory brainstem response (ABR) (B) at 1 kHz shown as a bubble chart (n=1 for small to n=4 for large). Compared to a slope of Panel A, the Panel B showed lower slope which had a correlation between higher thresholds in ABR and lower thresholds in PTA.
The threshold of the click-evoked BC ABR measurement was 31.25 dBnHL (SD, 10.24) for 20 subjects. However, no correlation was found between BC direct thresholds at 0.5, 1, 2, and 4 kHz and click-evoked ABR thresholds: r=0.199, p=0.401; r=0.222, p=0.348; r=0.284, p=0.225; and r=-0.044, p=0.855, respectively.
Discussion
While comparing the threshold of BC direct with those of behaviorally measured BC PTA and objectively measured BC ABR for 20 subjects with normal hearing, the present study aimed to determine the reliability of the BC direct thresholds and confirm the clinical feasibility through their relationships for application to young or older patients who have passive behavioral responses.
As expected, the BC PTA showed the lowest thresholds across the frequencies, whereas the BC ABR had the highest thresholds. Our results showed that the threshold difference of the four-tone average between BC PTA and BC ABR was approximately 28 dB. This finding was supported by Muchnik, et al. [10] and Seo, et al. [15]. However, in previous studies, the average threshold of subjects with normal hearing was approximately 18-19 dBnHL in the BC ABR measurement, and thus the threshold difference betwen BC PTA and BC ABR was 18 dB, which indicates that our study had an approximately 10 dB higher threshold than those in previous studies on BC ABR. One possible reason for this discrepancy is the unpleasant pressure and pain caused by the bone vibrator while measuring the BC ABR thresholds, even with no difference in the experimental conditions.
One striking finding of the present study is that the BC direct provided the differentiated threshold pattern in terms of frequency. In other words, there were low (or better) thresholds in the low frequencies, such as 500 and 1,000 Hz, and high (or worse) thresholds in the 2,000 and 4,000 Hz frequencies. However, as shown in Fig. 1, the group average of the 500 Hz thresholds was at least 5 dB worse than that of the 1,000 Hz thresholds. Hodgetts, et al. [16] explained this as inherent low frequency noise of the BAHA because the inherent noise masks the aided thresholds at 250 and 500 Hz. This was also supported by Pfiffner, et al. [17] in that physical characteristics of the sound processor provided a maximal output force at approximately 1 kHz. If this statement extends to our correlation results, it would be a strong finding with a significantly positive correlation between PTA and BC direct and between PTA and ABR at 1 kHz. Christensen, et al. [18], who estimated the BC direct thresholds of the subjects with a BAHA softband, showed that BC direct thresholds were 6-14 dB higher than BC PTA thresholds, while supporting our results of 3.81 dB for BC PTA and 16.37 dB for BC direct. Additionally, their post hoc results were in accordance with our findings that the thresholds of BC direct at 1 kHz were better than those at 500 or 4,000 Hz. This is a possible result when considering the transmission characteristics of the ear [18].
Nevertheless, the BC direct thresholds seemed large up to 20 dB at four testing frequencies, although another study achieved similar results of a 17.5 dB maximum difference at 2,000 Hz. This may be a possible limitation of the current study, which evaluated the individual with normal hearing with a BAHA softband. Therefore, we need to thoroughly investigate BC auditory pathways in a follow-up study. It is well known that the osseo-tympanic route (with sound radiated into the external ear canal, compression, and expansion of the petrous bone that results in displacement of fluid into the cochlea, and consequently basilar membrane motion) and the inertial effect of the middle ear ossicles and inner ear fluids constitute the most common measurements [19]. However, no studies have reported on the best dominant BC pathway in terms of force prorogation and loss. Therefore, the BC direct might be predictable at approximately 5 dB higher (or worse) than the BC PTA and 5-10 dB lower (or better) than the BC ABR in individuals with normal hearing, although a large data set is required for standardization. Further research should be conducted to gather data from patients with hearing impairment, including BAHA candidates/users for comparison between normal and pathological difference of the BC route and thresholds.
Acknowledgements
This work was supported by the National Research Foundation of Korea grant (NRF 2019K1A3A1A47000527).
Notes
Conflicts of interest
The authors have no financial conflicts of interest.
Authors’ contribution
Conceptualization: Woojae Han. Data curation: Yeoju Kim and Sihun Park. Formal analysis: Sunghwa You and Chanbeom Kwak. Funding acquisition: Youngjoon Seo. Methodology: Sihun Park, Yeoju Kim, and Woojae Han. Project administration: Chanbeom Kwak. Supervision: Woojae Han. Validation: Youngjoon Seo and Jihyeon Lee. Visualization: Yeoju Kim and Sunghwa You. Writing—original draft: Yeoju Kim. Writing—review and editing: All authors.