Comparison of Autophagy mRNA Expression between Chronic Otitis Media With and Without Cholesteatoma
Article information

Abstract
Background and Objectives
Autophagy is known to be associated with pathogen infection. However, the expression of autophagy-related proteins has not been studied in chronic otitis media without cholesteatoma (COM) or with cholesteatoma (CholeOM). This study aimed to determine whether there is a difference between COM and CholeOM in autophagy-related gene mRNA expression.
Subjects and Methods
For 47 patients with chronic otitis media, the inflammatory tissues were classified into granulation tissue (COM) or cholesteatoma (CholeOM) according to biopsy results.
Results
PI3K mRNA expression (COM vs. CholeOM, mean±SD, 0.009±0.010 vs. 0.003±0.004; p=0.004) was lower, whereas Beclin-1 mRNA expression (0.089±0.107 vs. 0.176±0.163; p=0.034) was higher in the CholeOM group. Expression of PI3K mRNA in the CholeOM group was lower than that in the COM subgroups with presence of bacteria (0.022±0.019 vs. 0.001±0.001; p=0.001), otorrhea (0.049±0.068 vs. 0.003±0.004; p=0.004), and hearing loss over 40 dB (0.083±0.130 vs. 0.003±0.004; p=0.005).
Conclusions
The data suggested that different autophagy proteins play important roles in chronic otitis media according to the presence or absence of cholesteatoma.
Introduction
Autophagy is a general term for lysosome-based mechanisms that break down targets in the cytoplasm. Autophagy can effectively remove cytosolic infectious pathogens directly through the lysosome or enhance phagocytosis of extracellular pathogens through the cell membrane. Autophagy is activated by infection with bacteria [1,2].
Middle ear infection is a general term applied to all inflammatory reactions in the middle ear showing pathological changes that involve bone destruction of structures as well as changes in the middle ear cavity and middle ear mucosal, epithelial, and subepithelial cells [3]. The cause of otitis media is complex and known to involve multiple factors, of which the most important are dysfunction of the eustachian tube and bacterial infection. After infection with bacteria, autophagy is activated and various immune responses are thought to be involved in the pathogenesis of chronic otitis media; however, not many studies have investigated the underlying mechanism.
A variety of different conditions and biochemical factors associated with the immune response are involved in various aspects of the development of inflammatory lesions in the middle ear cavity, and these processes are responsible for the recurrence and chronicity of otitis media [4-6]. The role of autophagy in chronic otitis media may be different depending on the presence or absence of accompanying cholesteatoma. It is likely that the mRNA expression of autophagy proteins differs according to clinical features and presence or absence of cholesteatoma, however, there is no reported study on this. Therefore, we investigated the expression pattern of autophagy-related mRNAs in chronic otitis media and compared expression levels according to the presence of cholesteatoma, bacterial infection, or otorrhea, as well as the degree of hearing loss.
Subjects and Methods
Subjects
The study population consisted of 47 patients who visited the Department of Otorhinolaryngology-Head and Neck clinic at a single tertiary medical center. Chronic otitis media was defined as the presence of persistent symptoms, such as hearing loss, otorrhea, tinnitus, and otalgia (±perforation of the tympanic membrane±otorrhea±attic destruction) lasting longer than 3 months, with the identification of a lesion on the middle ear and mastoid process on temporal bone computed tomography (TBCT). The presence or absence of otorrhea was confirmed with otoscopy and endoscopy; pus culture was conducted if otorrhea was observed in the external ear canal or tympanic membrane of the middle ear. The presence and severity of hearing disturbance was assessed with pure tone audiometry (PTA), preoperative TBCT was performed to assess the presence and severity of middle-ear lesions, and inflammatory tissue was obtained for biopsy during surgery to confirm the diagnosis of chronic otitis media. Chronic inflammation, granulation tissue, and cholesteatoma were identified with histologic biopsy of the middle ear inflammatory tissue. Based on results of histologic biopsy, the chronic otitis media patients were divided into the chronic otitis media without cholesteatoma (COM) group (presence of chronic inflammation and granulation tissue without cholesteatoma) and the chronic otitis media with cholesteatoma (CholeOM) group (presence of cholesteatoma).
We received prior permission for use of patient samples with written informed consent from the patients or their parents or guardians, and explained the purpose of the experiment to them. Patients who were suspected of having acute otitis media, otitis media with effusion, head and neck anomalies, systemic diseases, or congenital or acquired immune deficiencies were excluded.
The study protocol was approved by the Institutional Review Board of KyungHee Medical Hospital (IRB 2017-12-030).
Bacterial culture
When otorrhea was observed in patients, the sample was taken and tested for bacterial culture. After cleansing of the external auditory canal, the otorrhea sample was aseptically collected using sterilized cotton while employing an antiseptic otoscope to prevent contact with the external auditory canal. All clinical samples were sampled using sterile cotton swabs (Xomed Trace Products, Jacksonville, FL, USA), which were immersed in Stuart transport medium. Solid blood agar and liquid thioglycolate medium (Hangang, Gun-po, Korea) were inoculated with these samples, and the cultures were incubated for 24 h at 35.8°C. Bacteria that formed colonies were identified by Gram staining and biochemical testing.
RNA extraction and real-time PCR procedures
Total RNA was purified from patient samples using TRIzol solution (Invitrogen, Carlsbad, CA, USA) following the manufacturer’s protocol. RNA was isolated from tissues using RNeasy Mini kit (Qiagen, Hilden, Germany). First-strand cDNA synthesis was performed with 1.5 μg of total RNA, which was transcribed to cDNA using a reverse transcription system with random hexamers (Promega; Madison, WI, USA) according to the manufacturer’s protocol. Real-time PCR was performed on a StepOnePlus real-time PCR system with Power SYBR Green PCR Master Mix (Applied Biosystems, Foster City, CA, USA). PCR was performed with 2 µL of cDNA in a 20 µL reaction mixture containing 10 µL of Power SYBR Green PCR Master Mix, 2 µL of primers, and 7 µL of PCR-grade water. The primer sequences used are from a previous study [7] and shown in Table 1. The reaction conditions were denaturation at 95°C for 10 min, followed by 40 cycles of 95°C for 15 s and 60°C for 1 min. The crossing points of the target genes with β-actin were calculated using the formula 2-(target gene-β-actin), and relative amounts were quantified.

Primer sequences for real-time PCR
Evaluation of level of hearing loss
PTA was performed by measuring air and bone conduction, with hearing calculated as the average of three frequencies (500, 1,000, and 2,000 Hz). Using the quartering method, the mean PTA value was divided into subgroups of PTA less than 40 dB and PTA greater than 40 dB.
Statistical analysis
To investigate the statistical significance of expression of autophagy-related mRNA in the cholesteatoma of CholeOM and the granulation tissue of COM, student’s t-test was used for normally distributed data, and Mann-Whitney U test was used for non-normally distributed data. Chi-square test and Fisher’s exact test were used in the comparison analysis of demographic data. IBM SPSS version 20 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. A p-value less than 0.05 was considered significant.
Results
Demographics and clinical characteristics of subjects
Among the 47 patients with chronic otitis media, 28 were in the COM group and 19 were in the CholeOM group. The COM group contained more bacterial culture-positive patients than the CholeOM group (COM vs. CholeOM, 64.3% vs. 21.1%; p=0.049). Comparison between the groups showed no difference in age, gender, affected side, type, or degree of hearing loss. Pseudomonas aeruginosa was the most frequently detected strain, followed by methicillin-resistant Staphylococcus aureus (MRSA), coagulase-negative Staphylococcus, Staphylococcus aureus, and Achromobacter xylosoxidans (Table 2).
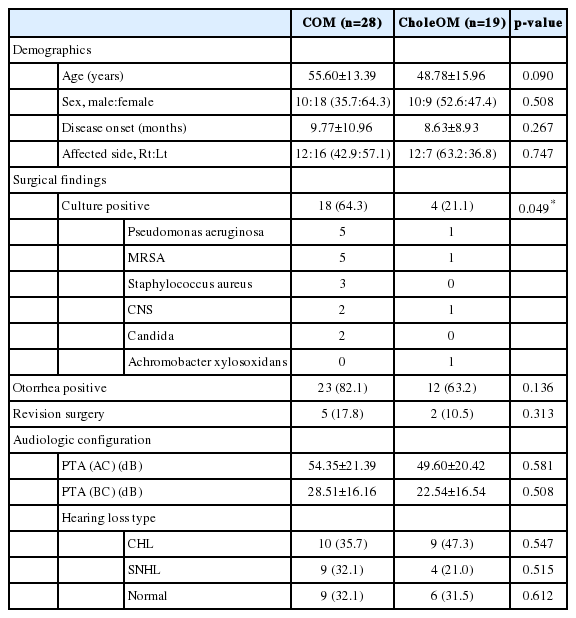
Demographic and clinical characteristics of patients with chronic otitis media without and with cholesteatoma
Expression of mTOR, P13K, LC3 II, Beclin-1, and Rubicon mRNAs
mTOR, P13KC3, LC3 II, Beclin-1, and Rubicon mRNA was expressed in skin, granulation tissue, and cholematrix obtained from all 47 patients. Expression of PI3K mRNA (COM vs. CholeOM, mean±SD, 0.009±0.010 vs 0.003±0.004; p=0.004) was lower and Beclin-1 mRNA (0.089±0.107 vs. 0.176±0.163; p=0.034) was higher in the CholeOM group (Table 3).
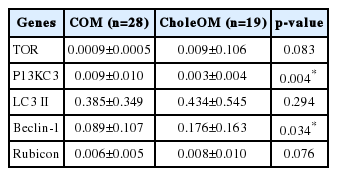
Expression of mRNA encoding autophagy-related proteins in chronic otitis media without and with cholesteatoma
Expression of mTOR, PI3K, LC3 II, Beclin-1, and Rubicon mRNAs in COM and CholeOM patients in the presence of bacteria
The expression of PI3K mRNA was lower in the CholeOM group than in the COM group when the bacterial culture was positive (COM vs. CholeOM, mean±SD, 0.022±0.019 vs. 0.001±0.001; p=0.001) (Table 4).
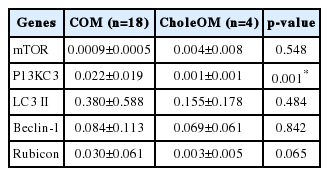
Expression of mRNA encoding proteins related to autophagy and ER stress in presence of bacteria in patients with chronic otitis media without and with cholesteatoma
Expression of mTOR, PI3K, LC3 II, Beclin-1, and Rubicon mRNAs in COM and CholeOM patients in the presence of otorrhea
In the presence of otorrhea, the expression of PI3K mRNA was lower in the CholeOM group than in the COM group (COM vs. CholeOM, mean±SD, 0.049±0.068 vs. 0.003±0.004; p=0.004) (Table 5).
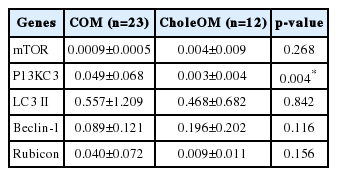
Expression of mRNA encoding proteins related to autophagy and ER stress in presence of otorrhea in patients without and with cholesteatoma
Expression of mTOR, P13KC3, LC3 II, Beclin-1, FLIP, Rubicon, BIRC2, and BIRC5 mRNAs in patients with over 40 dB hearing loss
PI3K mRNA expression was significantly lower in the CholeOM group than in the COM group when the hearing loss was more than 40 dB (COM vs. CholeOM, mean±SD, 0.083±0.130 vs. 0.003±0.004; p=0.005) (Table 6).
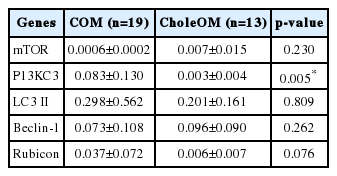
Expression of mRNA encoding autophagy-related proteins in patients with over 40 dB hearing loss without and with cholesteatoma
Discussion
Autophagy may be involved in the turnover of essential cytoplasmic components or may be induced by external environmental changes such as depletion of nutrients or pathogen invasion. It is also involved in the differentiation and development of tissues and is reported to play a role in diseases such as cancer, muscular disorders, neurodegeneration, and pathogen infection [2,8,9]. Autophagy is associated with cell survival, energy maintenance, and metabolic generation in metabolic diseases, with apoptosis in pulmonary diseases, aggregate clearance and mitochondrial preservation in neurodegenerative diseases and aging, and cell death, chemosensitization, tumor suppression, chemoresistance, radioresistance, and tumor growth in cancers. Autophagy was also shown to be associated with plaque stabilization and regulation of proliferation in vascular diseases and with antigen preservation, pathogen removal, regulation of inflammation, and viral replication in infectious diseases [8,10,11]. Therefore, it is likely that autophagy also plays a role in the pathogenesis of chronic otitis media, which is closely related to bacterial infection.
The autophagy process involves several steps, which are classified somewhat differently by various authors but can be broadly divided into initiation, vesicle nucleation, vesicle elongation, fusion, degradation, and termination [12,13]. In the present study, we could not study all of the mRNAs associated with autophagy because the number of cells in the samples collected from of the otitis media cases was insufficient. Therefore, we selected mTOR related to initiation, PI3K and Beclin-1 related to vesicle nucleation, LC3 II related to vesicle elongation, and Rubicon related to fusion and degradation. These autophagy-related mRNAs were expressed in both COM and CholeOM groups, even when patients were divided according to detection and non-detection of bacteria, indicating an immune response to bacterial infection. Our results showed that autophagy was involved in all chronic otitis media cases regardless of whether cholesteatoma was present.
The biological role of autophagy is different according to activated or inactivated disease [14-16]. Especially, in pathogen infection, activation of autophagy leads to cellular defense against invasive bacteria and viruses, and inactivation of autophagy allows pathogens to establish a replicative niche. This study did not reveal the role of autophagy in activation and inactivation of COM because we only analyzed the expression patterns of autophagy-related mRNAs in the presence or absence of cholesteatoma and according to clinical manifestations. However, different autophagy-related mRNAs were expressed at different levels between the COM group and CholeOM group. We cannot explain why PI3K mRNA, associated with vesicle nucleation, was expressed at a lower level in the CholeOM group, or why expression of Beclin-1 mRNA was lower in the COM group. Vesicle nucleation during the autophagy process may play an important role in the pathogenesis of chronic otitis media, and even though the same vesicle nucleation process occurs, various autophagy proteins may play different roles depending on the presence of granulation tissue in COM and cholesteatoma in CholeOM.
Activation of phosphoinositide 3-kinase (PI3K) by various factors, such as tumorigenic genes, growth factors, and growth factor receptors, is considered to be a characteristic of cancer. PI3K regulates the development, differentiation, growth, proliferation, and activation of various immune cells that are highly involved in the pathogenesis of innate immune and acquired immune-mediated diseases [17]. However, the role of PI3K in chronic otitis media has not been elucidated. The expression of PI3K in all samples of this study strongly indicated involvement in the pathogenesis of chronic otitis media. Beclin-1 not only activates autophagy, but also inhibits tumorigenesis. Mice with disruption of the Beclin-1 gene have a higher incidence of lymphoma, lung cancer, and liver cancer [17]. A recent study also showed that Beclin-1 is associated with the onset and chronicity of otitis media with effusion [7]. Further studies investigating the effects of PI3K and Beclin-1 mRNA expression on the progression, recurrence, chronicity, and degree of hearing loss in otitis media patients are necessary.
Major pathologic findings in the middle ear cavity in chronic otitis media patients include formation of granulation tissue, cholesterol granuloma, cholesteatoma, fibrosis, and changes in bone formation. In this study, the granulation tissue of COM patients was induced by inflammation caused by middle ear exudates and changes in epithelial cells and subepithelial tissue of the middle ear mucosa. Cellular components were abundant in the acute and subacute phases of otitis media, whereas fibrous tissue was abundant in the chronic phase [18-20]. In the CholeOM group, cholesteatoma was characterized by invasive growth of keratinized stratified squamous epithelium into mucosa in the middle ear cavity, destroying the surrounding bone tissue through accumulation of keratin and resulting in more severe and serious complications than in the COM group. Bone destruction involves various enzymes, such as collagenase, acid phosphatase, and acid protease secreted from the inflammatory and granulation tissue, and by the pressure effect of the cholesteatoma itself [18,21-23]. Recently, several types of cytokines secreted from inflammatory cells have been shown to be involved in these actions [24-27]. The results of the present study indicate that autophagy is also involved. The granulation tissues observed in the COM group and the cholesteatoma tissues observed in the CholeOM group induce inflammation in normal tissues, suggesting that the inflammatory response is inevitably related to autophagy gene expression.
The bacterial culture test in chronic otitis media is a necessary test for selecting appropriate antibiotics. In this study, P. aeruginosa was detected most frequently in bacterial culture tests of otorrhea, followed by MRSA, coagulase-negative Staphylococcus, S. aureus, and A. xylosoxidans. In both COM and CholeOM groups, complex infections with aerobic and anaerobic bacteria were the most common, with rates as high as 50%. The most common aerobic bacteria were P. aeruginosa, and the bacterial culture test results of this study were consistent with those of a previous report [28,29].
In general, the extent of otorrhea in CholeOM is often less than that in non-cholesteatoma otitis, especially in the initial state of epitympanic recess retraction. A large extent of otorrhea indicates that a secondary bacterial infection has occurred. However, in the present study, the detection rate of bacterial growth in pus culture was statistically higher in the CholeOM group than in the COM group. These results suggest that patients in the CholeOM group did not visit the hospital because the incidence of otorrhea was low; however, it is also possible that, when patients did visit the hospital due to severe otorrhea, the inflammatory reaction induced by bacteria was severe, which indicated that the CholeOM group had a higher positive rate than the COM group. Further studies will be necessary to determine whether PI3K mRNA expression inhibits the development of otorrhea, whether PI3K is active in the granulation tissues rather than cholesteatoma or otorrhea caused by inflammation of the middle ear, and whether the low expression of PI3K mRNA in the CholeOM group compared with the COM group in the presence of otorrhea and in the culture-positive group is related to vigorous bacterial growth.
Hearing loss is one of the most common symptoms of chronic otitis media. In the present study, the expression of PI3K mRNA was significantly lower in the CholeOM group than in the COM group in the presence of hearing loss greater than 40 dB, suggesting that PI3K mRNA may be involved in severe middle ear lesions in the CholeOM group. The degree of hearing impairment is determined by a combination of the size of the tympanic membrane perforation, ossicle conditions, severity of the middle ear inflammation, presence or absence of otorrhea, and inner ear involvement [30]. Therefore, although it is difficult to conclude that the PI3K expression was related to hearing loss, this association is indirectly supported by the difference in mRNA expression according to the presence of cholesteatoma.
There are some limitations to this study. First, this study was performed only at the mRNA level, and data at the protein level are not available. Second, patients who were classified as the otorrhea-negative group had no otorrhea in the external auditory canal when they visited the hospital, although they had experienced otorrhea in the past. Third, there was a possibility that prophylactic use of antibiotics to reduce inflammation affected bacterial culture and expression of autophagy-related mRNA in both otorrhea-positive and -negative groups. Fourth, we could not elucidate why expression of PI3K and Beclin-1 mRNA was significantly different between COM and CholeOM groups among the many autophagy-related mRNAs.
In summary, among the various autophagy-related mRNAs studied, expression of PI3K mRNA was significantly lower in the CholeOM group, and that of Beclin-1 mRNA was significantly lower in the COM group, suggesting that different autophagy proteins play important roles in chronic otitis media according to the presence or absence of cholesteatoma.
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (NRF-2018 R1A6A1A03025124).
Notes
Conflicts of interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Seung Geun Yeo. Data curation: Su Young Jung, Young Il Kim, Sang Hoon Kim. Formal analysis: Su Young Jung, Sang Hoon Kim. Funding acquisition: Sang Hoon Kim, Seung Geun Yeo. Investigation: Seung Geun Yeo. Methodology: Young Il Kim, Seung Geun Yeo. Project administration: Junyang Jung, Su Young Jung. Resources: Young Il Kim, Sang Hoon Kim, Seung Geun Yeo. Software: Su Young Jung, Myung Gu Kim, Young Il Kim. Supervision: Seung Geun Yeo. Validation: Seung Geun Yeo. Visualization: Junyang Jung, Seung Geun Yeo. Writing—original draft: Junyang Jung, Seung Geun Yeo. Writing—review & editing: Seung Geun Yeo. Approval of final manuscript: all authors.