Analysis of Effect of Eggshell Membrane Patching for Moderate-to-Large Traumatic Tympanic Membrane Perforation
Article information
Abstract
Background and Objectives
To evaluate the effect of eggshell membrane (ESM) patching for tympanic membrane (TM) perforation, and to investigate correlations between healing time and age, gender, patching time, perforation size, and perforation location.
Subjects and Methods
One hundred and seventy-five patients diagnosed with traumatic TM perforation at the Department of Otorhinolaryngology-Head and Neck Surgery, Korea University Ansan Hospital, between January 2008 and October 2013. Patients were divided into two groups, according to perforation edge approximation or ESM patching treatment. Healing time was compared between the group that received perforation edge approximation and the group that received ESM patching. Perforation grade, age, onset, and location were also compared between the two groups.
Results
ESM patching significantly improved healing time compared to spontaneous healing, especially in patients with moderate or large traumatic TM perforations (≥grade II). However, patient age, gender, perforation location, and especially timing of procedure, did not significantly affect healing time.
Conclusions
ESM patching can be a good treatment choice to promote tympanic membrane healing in large traumatic TM perforations.
Introduction
The tympanic membrane (TM) divides the external ear and the middle ear. Its function is to perceive sound, and it is greatly sensitive to changes in external auditory canal air pressure. Sudden powerful forces to the ear, such as may be caused by hand, object, or car accident, can cause increased ear canal air pressure. Traumatic TM perforation is routinely observed in our otolaryngology outpatient clinic.
It is well established that most traumatic TM perforations tend to close spontaneously (76-94%) [123456]. However, those that fail to heal can result in moderate-to-large perforations. A majority of otolaryngologists agree that performing early myringoplasty can improve healing rate [78]. However, this procedure involves risk, cost, and the inconvenience of an operation. Therefore, a non-surgical procedure, such as patch application, is usually selected as initial treatment. Various patching materials have been proposed, including paper, silk, gelatin sponge, fibroblast growth factor, insulin-like growth factor, chitosan, and human urinary bladder. However, the benefits and duration of each material are controversial [19].
Eggshell membrane (ESM), routinely used in wound dressings, is another potential patching materials [10]. In a previous study, we reported that the healing ratio of the TM was not significantly different between the ESM patch group and the edge approximation group, but that healing time was significantly shorter in the ESM patch group [10]. The present study had two main objectives: 1) to investigate the effect of ESM patching of traumatic TM perforation, according to the Griffin's TM perforation grade, and 2) to compare healing time according to the patching time, perforation location, and age in the ESM patch application group.
Subjects and Methods
Data source and study population
This is a retrospective review of 175 patients diagnosed with traumatic TM perforation at the Department of Otorhinolaryngology-Head and Neck Surgery, Korea University Ansan Hospital, between January 2008 and October 2013. Exclusion criteria were as follows; patients with temporal bone fracture, disruption of ossicles, previous perforation, or incomplete closure.
The external auditory canals of all 175 ears were cleaned when the patients visited the hospital, and the location and size of the perforation were recorded by ear endoscopy. Pure tone audiometry was performed before treatment.
TM perforation size was evaluated by Griffin's criteria [11] and graded into four categories, as follows, grade I=perforation involved ≤25% of the pars tensa, grade II=perforation involved 25-50% of the pars tensa, or multiple perforations involved two quadrants, grade III=perforation involved 50-75% of the pars tensa, or multiple perforations involved three quadrants, and grade IV=perforation involved 75-100% of the pars tensa [11]. The study was approved by the institutional review board of Korea University College of Me-dicine, and conducted according to the principles expressed in the Declaration of Helsinki (AS10131-001).
Treatment selection
ESM patch (n=111) or approximation (n=64) was randomly selected for treatment of the traumatic TM perforation by the patients physician. Oral antibiotics were administered for 1 week to prevent infections. Patients were regularly followed-up at the outpatient clinic until the TM perforation was closed. Perforation closure was confirmed by endoscopic examination.
ESM patch group
The eggs used for ESM patches were obtained from a traditional market. Eggs were washed with distilled water and brushed with a nylon brush. Eggs were then boiled in distilled water for 5 min, broken, and the egg content was emptied. The remaining hard eggshell with membrane was washed with distilled water and the membranes were carefully extracted by hand. The extracted ESM was cut to make a round disc with a skin puncture. The final ESM patch diameter was 5 mm. ESM patches were sterilised with ethylene gas [10]. During the ESM patch application, flaps of the perforation were approximated where possible and the ESM patch was placed in saline for moistening before application. The operator placed the ESM patch on the lateral surface of the perforation with the guidance of a microscope, and then ensured that it adhered to the TM [10]. The ESM patch was retried to 3 times during 3 months. After the ESM patch was removed spontaneously, tympanic membrane was evaluated.
Approximation group
Under an otomicroscope, EMLA® cream (lidocaine 2.5% and prilocaine 2.5%; Astrazeneca AB, Karlskoga, Sweden) were applied into the EAC for 10 minutes. The inverted edges were aligned back to the original position as much as possible using a Rosen needle or a vacuum suction tip, however no patching materials were used.
Statistical analysis
All data are expressed as mean±standard deviation (SD). We used independent T-tests for healing time according to treatment method, age, and time. In addition, we performed analysis of variance (ANOVA) for comparing healing time according to location of TM perforation using SPSS software version 21 (IBM SPSS Inc., Chicago, IL, USA). Differences were considered statistically significant when p<0.05.
Results
In the 175 ears with traumatic TM perforation, 111 (62.6%) were to the left ear and 64 (37.4%) were to the right ear. Mean patient age was 27.6±16.6 years and the mean air-bone gap was 16.2±10.1 dB. The number of patients with grade I perforation was 103, grade II was 49, grade III was 21 and grade IV was 2, as shown in Fig. 1.

Distribution of two groups according to Griffin's grade. There were 41 approximation patients and 62 ESM patch application patients with grade I perforation, 17 approximation patients and 32 ESM patch application patients with grade II perforation, 5 approximation patients and 16 ESM patch application patients with grade III perforation, and 1 approximation patient and 1 ESM patch application patient with grade IV perforation. ESM: eggshell membrane.
Healing time analysis between the ESM patch group and the approximation group included 103 patients with small traumatic TM perforation (grade I) and 72 patients with moderate-to-large traumatic TM perforation (≥grade II). Characteristics of the two groups are compared in Table 1. The mean perforation closure times were 37.3±24.5 in the approximation group and 36.4±26.4 days in the ESM patch group in patients with small traumatic TM perforation. Complete closure time was not statistically different between the 2 groups (p=0.205). However, in patients with moderate-to-large traumatic TM perforation, the mean perforation closure times was 110.4±127.4 in the approximation group and 77.4±78.6 days in the ESM patch group. Healing time was significantly shorter in the ESM patch group than in the approximation group in patients with moderate-to-large traumatic TM perforation (p=0.007) (Fig. 2).

Summary of patient characteristics in the approximation group and the ESM patch group

Healing time in the ESM patching group and the approximation group according to TM perforation grade. The mean perforation closure times were 37.3±24.5 in the approximation group and 36.4±26.4 days in the ESM patch group in patients with small traumatic TM perforation. Complete closure time was not statistically different between the 2 groups (p=0.205). However, in patients with moderate-to-large traumatic TM perforation, the mean perforation closure times was 110.4±127.4 in the approximation group and 77.4±78.6 days in the ESM patch group. Healing time was significantly shorter in the ESM patch group than in the approximation group in patients with moderate-to-large traumatic TM perforation (p=0.007*). *statistically significant. ESM: eggshell membrane, TM: tympanic membrane.
TM closure time was analysed in 111 patients with ESM patching for TM perforation, according to age, patching time, and perforation location. The mean TM closure time was 58.5±23.9 days for non-adult patients (≤18 years) and 56.4±14.7 days for adult patients (>18 years). There was no significant difference in TM closure time between non-adult patients and adult patients (p=0.591) (Fig. 3).
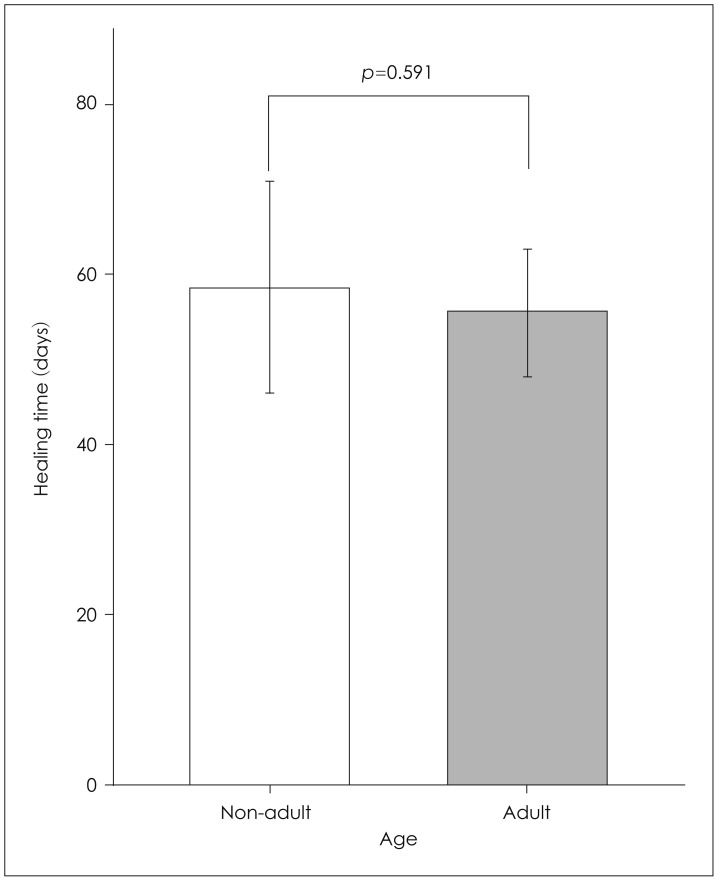
Healing time in ESM patching patients according to patient age group. The mean healing time was 58.5±23.9 days in non-adult patients (≤18 yrs) and 56.4±14.7 days in adult patients (>18 yrs). This result was not significant (p=0.591). ESM: eggshell membrane.
The mean TM closure time was 54.8±34.7 days for early patching patients (<1 week post injury) and 62.3±39.6 days for late patching patients (≥1 week post injury, p=0.326). In the small TM perforation patients, there was no significant difference in healing time between the early patching group and the late patching group (p=0.419) (Fig. 4). The mean TM closure time was 54.9±21.6 days for patients with anterior inferior quadrant TM perforation, 63.4±42.3 days for patients with anterior superior quadrant TM perforation, 55.3±24.2 days for patients with posterior inferior quadrant TM perforation, and 70.2±76.5 days for patients with posterior superior quadrant TM perforation (p=0.252) (Fig. 5).
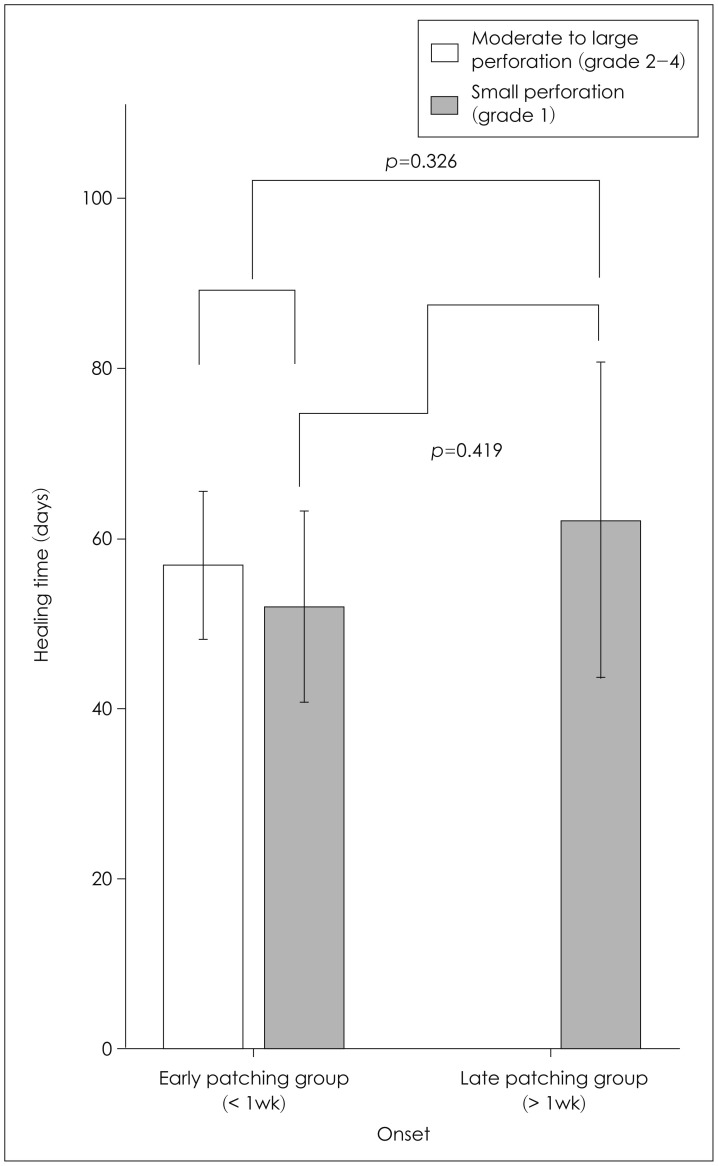
Healing time in early patching group and late patching group according to TM perforation grade. The mean TM closure time was 54.8±34.7 days for early patching patients (<1 week post injury) and 62.3±39.6 days for late patching patients (≥1 week post injury, p=0.326). In the small TM perforation patients, there was no significant difference in healing time between the early patching group and the late patching group (p=0.419). TM: tympanic membrane.
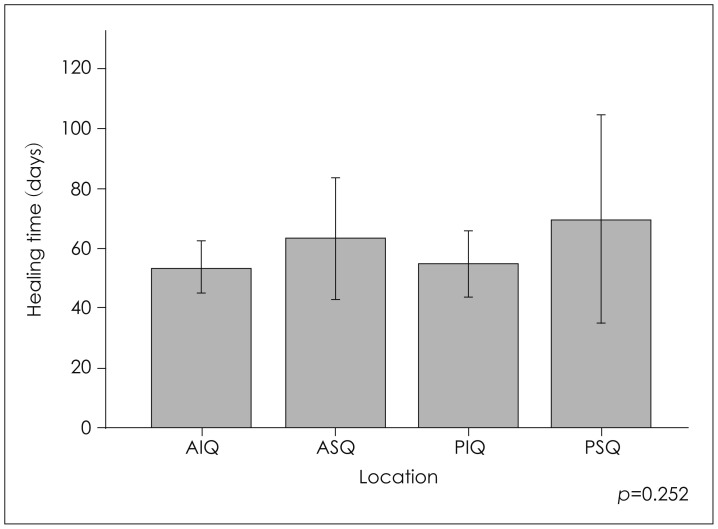
Healing time according to location of TM perforation in ESM patching patients. The mean TM closure time was 54.9±21.6 days for patients with AIQ TM perforation, 63.4±42.3 days for patients with ASQ TM perforation, 55.3±24.2 days for patients with PIQ TM perforation, and 70.2±76.5 days for patients with PSQ TM perforation. There were no significant differences (p=0.252, ANOVA). AIQ: anterior inferior quadrant, ASQ: anterior superior quadrant, PIQ: posterior inferior quadrant, PSQ: posterior superior quadrant, ESM: eggshell membrane, TM: tympanic membrane.
Discussion
Traumatic TM perforation is commonly observed in our otolaryngology outpatient clinics. Ear fullness, conductive hearing loss, middle ear infection, continued inflammation, and further tissue damage may result from continuous TM perforation [41112]. Fortunately, most traumatic perforations heal spontaneously [123456]. However, failure of complete closure and delayed TM perforation closure can occur in some cases. It has been suggested that curled edges of the perforated site edge cause the failure of complete spontaneous healing [126].
In our previous study, a patch-applied group was compared with an edge-approximated group for TM perforation, and we reported that an ESM patch did not affect healing rate [10]. However healing time was shorter in the patch application group [10]. The present study included almost 4 times more patients, affording results that are more definitive. In addition, we conducted further research in to the relationship between healing time and Griffin's grade, age, patching time, and perforation location.
Various materials are available for TM perforation patch application, including gentamicin ointment plugs, paper, tape, silk, water-soluble chitosan, alloderm, urinary bladder matrix, and growth factor combined patches [1314151617]. ESM patches have several advantages over the use of other materials, including anti-infection properties, water insolubility, similar physical properties to the TM for sound conduction, and low cost [181920].
In the current study, we show that ESM patching reduces healing time compared with edge approximation only, especially in patients with moderate or large traumatic TM perforation (≥grade II). Small TM perforations have high healing rates and short closure times, without any intervention [12].
Our study also showed that there was no significant difference between early patching (less than 1 week after injury) and late patching (more than 1 week after injury) in patients with ESM patching group. We assume that late patching has a similar effect on healing time. However, no patients with moderate or large TM perforations received ESM patching more than 1 week after injury, therefore further studies are required in this patient group. In addition, healing time was not affected by age or perforation location.
In conclusion, ESM patch application in patients with moderate or large traumatic TM perforation (≥grade II) is beneficial for reducing healing time and avoiding infection at any time post-injury, at any age, or at any tympanic membrane injury site.
Acknowledgments
This work was supported by the Daewoong Pharmaceutical Co. LTD (AS10131-001).
Notes
Conflicts of interest: The authors have no financial conflicts of interest.