Introduction
Complications during aural impression-taking for hearing aids are relatively rare. There are several reports in the literature of complications related to ear mold impression material [123456]. Most cases occurred when there was preexisting perforation of the tympanic membrane, although traumatic perforation occurred in rare cases. While impacted mold material in the open mastoid cavity or external ear canal can be easily removed without complications, removal of the foreign body from the middle ear is challenging and should not be undertaken by inexperienced operators.
To date, transcanal or meatoplasty are the most commonly used approaches. However, a dumbbell-shaped mass impacted in the middle ear cavity cannot be removed by transcanal approach. Furthermore, while symptoms and surgical treatment for impression material in the middle ear have been reported [12345678], a case of impression material in the middle ear with accompanying methicillin-resistant Staphylococcus aureus (MRSA) otorrhea has not. We have experienced a case of silicone impression material in the middle ear with MRSA otorrhea.
We report the findings for a 74-year-old man who suffered intractable pulsating purulent discharge with otalgia following fitting of the silicone mold for a hearing aid. A large amount of silicone impression material thus impacted the middle ear like an iceberg. After topical treatment of the MRSA otorrhea by vancomycin otic solution and diluted vinegar solution irrigation, we removed the impression material using canal wall-up mastoidectomy. We present here our review of the literature regarding such a case.
Case Report
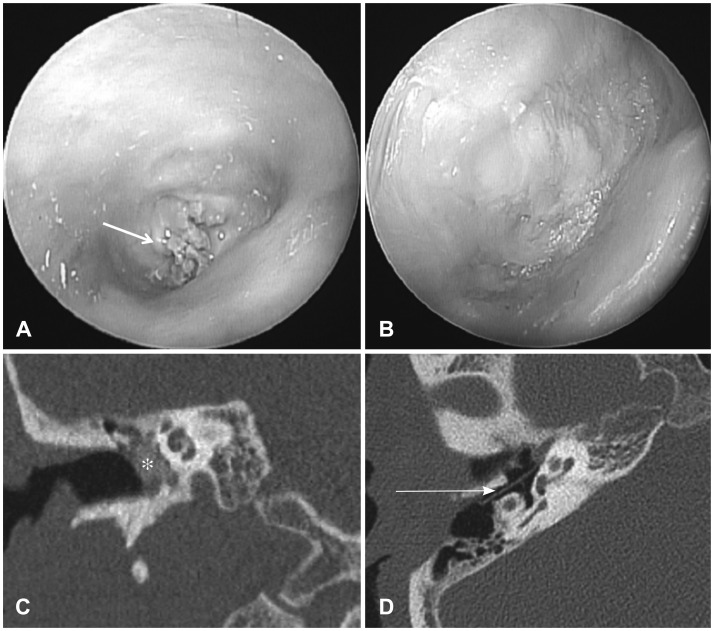
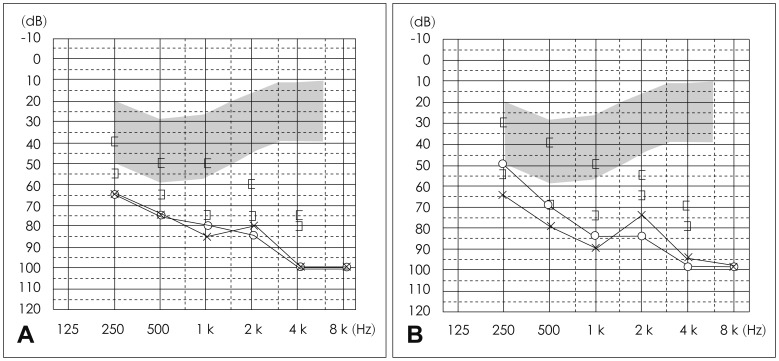
Several days after being diagnosed with simple chronic otitis media without otorrhea at the local clinic, he visited a local shop selling hearing aids. After hearing aid molding was performed, the mold could not be removed. Ten days after hearing aid fitting, patient had severe otalgia, aggravated hearing loss, and dizziness. Otomicroscopic examination found pulsating purulent discharge with blue mold material from the middle ear (Fig. 1A). The pulsating discharge was collected using a swab for the pus culture and antibiotic sensitivity test, which revealed MRSA. Temporal bone CT showed the soft tissue in the middle ear encasing the ossicle (Fig. 1C). Pure tone audiogram (PTA) showed moderate to severe mixed hearing loss in the right side and severe sensorineural hearing loss in the left side (Fig. 2A).
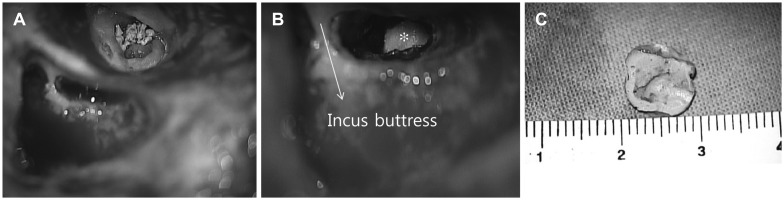
The patient was treated for MRSA otorrhea as an outpatient with diluted vinegar irrigation (vinegar: distilled water =1:2) and topically prepared otic solution of vancomycin. A 500-mg vial of vancomycin powder was reconstituted with 30 mL of sterile distilled water. The prescribed dose of vancomycin was two drops (0.8 mg) applied topically to the ear, three times daily for a total of 14 days. After 7 days, the pulsating otorrhea continued to resolve, with the most remarkable improvement occurring by day seven of the 7-day treatment period. Three weeks after the otorrhea ceased, removal of the impression material was not achieved by transcanal approach. Afterall, the removal accomplished via a canal wall-up mastoidectomy with posterior tympanotomy approach to the middle ear (Fig. 3A, B). Silicone impression material was visible via the facial recess and was complicated by encirclement of the ossicles by the material. After removal of the granulation tissue around the ossicle, the silicone material could be removed (Fig. 3C). The ossicle was left intact. The tympanic membrane perforation was reconstructed by temporalis fascia. Silastic sheet insertion from the mastoid to the middle ear via posterior tympanotomy was performed for ventilation. Vancomycin impregnated Gelfoam (Pharmacia & Upjohn, Kalamazoo, MI, USA) was packed in the middle ear for prevention of infection. The fascia was epithelized within the first month (Fig. 1B), and the valsalva maneuver was positive. Five months later, postoperative temporal bone CT showed well ventilated middle ear and mastoid cavity (Fig. 1D). The postoperative PTA showed mildly improved bone conduction compared to preoperative PTA (Fig. 2B). The patient has worn behind-the-ear digital hearing aids in both sides.
Discussion
Fitting a hearing aid usually requires the making of an ear mold. The silicone impression material is commonly used. Although this procedure is not difficult, otoendoscopic evaluation is needed to find lesions of the external canal and the tympanic membrane perforation [5]. In the present study, the hearing aid specialist did not detect the tympanic membrane perforation before the patient underwent hearing aid fitting. Therefore, molding into the middle ear and it was not removed. To date, there have been 27 reported cases of impression material foreign bodies. However, intractable MRSA otorrhea combined with impression material foreign body has not been reported. There has been a steady increase in the number of cases of otorrhoea caused by MRSA [8]. Vancomycin is the drug of choice in treating MRSA-infected patients. Topical otic solution has an advantage because of higher levels of antibiotic in the middle ear compared to systemic injection [9]. In the present study, we treated patients with MRSA otorrhea as outpatients using a topically prepared otic solution of vancomycin with diluted vinegar irrigation.
These days, severe complications of otitis media are rare today. The availability and use of antibiotics has significantly decreased the incidence of intratemporal and intracranial complications of otitis media in south Korea. Labyrinthitis induced the most profound inner ear damage, and therefore it was the single most disabling form of intratemporal complications. Symptoms, aggravated hearing loss and vertigo were frequently encountered. The patients with labyrinthitis developed severe hearing loss or deafness. In the present study, patient did not show nystagmus and the dizziness improved immediately after administering antihistamine medication. Ahlthough his hearing was subjectively worse on the right side before undergoing hearing aid fitting. However, causal relationship was established due to lack of pre-complication audiograms.
Most reported patients had either conductive, mixed, or sensorineural hearing loss, due to the foreign body and/or extraction surgery. In this particular case, the patient had preexisting mixed hearing loss at the right side and sensorineural hearing loss at the left side. The hearing deterioration occurred due to the foreign bodies at the right side. Silicone impression was removed by transcanal sharp dissection with success [123456]. However, this often requires disrupting the continuity of the ossicular chain to completely remove the material if this has not previously occurred secondary to erosion from the mold material [12].
In the present case, the silicone impression material was removed by canal wall-up mastoidectomy. Through the facial recess, the ossicle was dissected from the silicone mold material. The granulation tissues were removed from the ossicle and middle ear mucosa. Although the MRSA discharge was stopped, the remaining biofilm on the granulation tissues could induce a postoperative infection and wound disruption. Therefore, we removed as much of the granulation tissue as possible. After irrigation with vancomycin diluted in saline, middle ear packing was performed using vancomycin solution impregnated gelfoam for prevention of postoperative infection. The patient showed no postoperative infection and the fascia graft dried up well. Five months later, postoperative temporal bone CT showed well ventilated middle ear and mastoid cavity.
In conclusion, if impression material in the middle ear causes infection, it can induce potential serious complications. Adequate preoperative treatment for otorrhea and delayed surgical treatment is necessary. In this study, we treated MRSA otorrhea by topical vancomycin otic solution and diluted vinegar irrigation. After otorrhea ceased, we removed the impression material by canal wall-up mastoidectomy. This case showed that otoscopic examination of the tympanic membrane perforation is important. If a tympanic membrane perforation is exists, presence of impression material in the middle ear can lead to complication during the procedure of hearing aid fitting. Therefore, through otoscopic examination is essential before undergoing hearing aid fitting. Further we recommend that hearing aid fitting should be performed by an otolaryngologist instead of a hearing aid specialist.