Introduction
Hearing impairment is one of the known causes of the global burden of disease [1]. Hearing impairment can cause an effect on social communication, psychosocial health, quality of life, and economic independence [1-3]. In children, hearing impairment leads to delays in speech and language development. There are two main types of hearing loss: sensorineural hearing loss (SNHL) and conductive hearing loss. SNHL results from damage to the cochlea, auditory nerve, or central nervous system. In the majority of SNHL patients, the lesion is in the cochlea (sensory). The lesion of the auditory nerve (neural) is uncommon and this cannot be differentiated from cochlear losses using clinical symptoms alone [2]. Further, the SNHL can also be unilateral, hearing loss in one ear and bilateral, wherein hearing loss is in both ears.
The differential diagnosis of various causes of SNHL is essential as lesion can happen at various structures, including injury to outer hair cells (OHCs), inner hair cells (IHCs), auditory dyssynchrony, and tumors in the cochlear vestibular nerve. This is a challenging task in unilateral SNHL. The differential diagnosis may be done using test battery approach. A test battery approach in audiological evaluation includes various diagnostic tests during the initial evaluation, including pure-tone audiometry, acoustic reflex testing, imaging, and auditory brainstem response (ABR) testing [3]. The importance of the test battery approach in knowing the exact site of lesion in a patient with unilateral hearing loss due to selective IHC lesion is highlighted in the present case study.
Case Report
A 14-year-9-month-old adolescent came to the Department of Audiology with the major complaint of reduced hearing sensitivity in the left ear. The patient also reported having difficulty in understanding speech from a distance for the past three months. A detailed case history was taken from the patient and her guardian. The condition was reported to be acquired in nature and there was no report of any other otological complaints. It was also noted that the patient was earlier diagnosed with minimal hearing loss in the right ear and severe SNHL in the left ear with the possible indication of auditory neuropathy spectrum disorder (ANSD) at a private hospital. Later, routine audiological evaluations, including pure tone audiometry, speech audiometry, and immittance evaluations, were done on the patient. A calibrated two channel diagnostic audiometer, MA-53 (MAICO Diagnostics, Berlin, Germany) equipped with TDH39 headphones was used to perform pure tone audiometry and speech audiometry. Results of the pure tone audiometry test showed that the patient had normal hearing sensitivity in the right ear (pure tone average [PTA]: 5 dB) and profound hearing loss in the left ear (masked PTA: 101.25 dB). Speech recognition thresholds (SRT) and speech identification scores (SIS) were assessed in speech audiometry. SRT was noted to be 5 dB for the right ear and 95 dB (masked) for the left ear. SIS of 100% and 8% (masked) was noted for right and left ear, respectively (Fig. 1A). Ethical guidelines recommended by AIISH bio-behavioral research involving human subjects were followed [4], and informed consent was taken from the guardian of the patient.
Immittance evaluation was done using GSI-TympStar (Grason-Stadler, Eden Prairie, MN, USA). Tympanometry showed an “A” type of tympanogram in both ears. Acoustic reflex results showed that the right ear ipsilateral (right ear: probe ear) and left ear contralateral (left ear: probe ear, right ear: phone ear) acoustic reflexes were present. However, the right ear contralateral (right ear: probe ear, left ear: phone ear) and left ear ipsilateral (left ear: probe ear) acoustic reflexes were elevated for 500 Hz and 1,000 Hz and absent for 2,000 Hz and 4,000 Hz. A calibrated ILOV6 OAE analyzer (Otodynamics Ltd., Hatfield, UK) was used for recording transient evoked otoacoustic emissions (TEOAEs) and distortion product (DP) OAEs. It was noted that the TEOAEs and DPOAEs were present in both ears, demonstrating normal OHC functioning (Table 1).
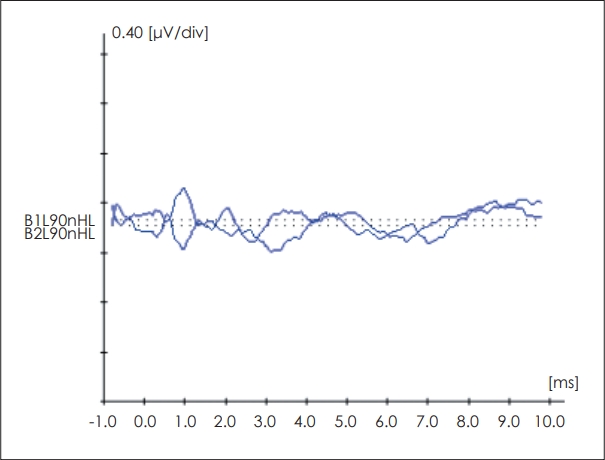
ABR test was done to confirm the behavioral thresholds and to understand the site of lesion testing. A calibrated Biologic Navigation Pro system (version 7.0.0; Natus Inc., Pleasanton, CA, USA) fitted with an ER-3A insert receiver was used for ABR recording. For the site of lesion testing, a double channel recording was done at two repetition rates of 90.1/s and 11.1/s with the click stimulus at 90 dB nHL. It was noted that the peaks I, III, and V were visualized in the right ear at normal latencies, and no peaks were visualized in the left ear. However cochlear microphonics (CM) could be seen in the left ear till around 5 ms (Fig. 2). Based on the above findings, provisional diagnosis was made as normal hearing sensitivity in the right ear and profound hearing loss in the left ear with possible indication of retrocochlear pathology. The patient was counseled for neurological consultation.
The patient reported back after two months for a follow-up evaluation with neurological reports. Reports of CT scan showed normal nerve VIII, brain parenchyma, and bilateral temporal bones.
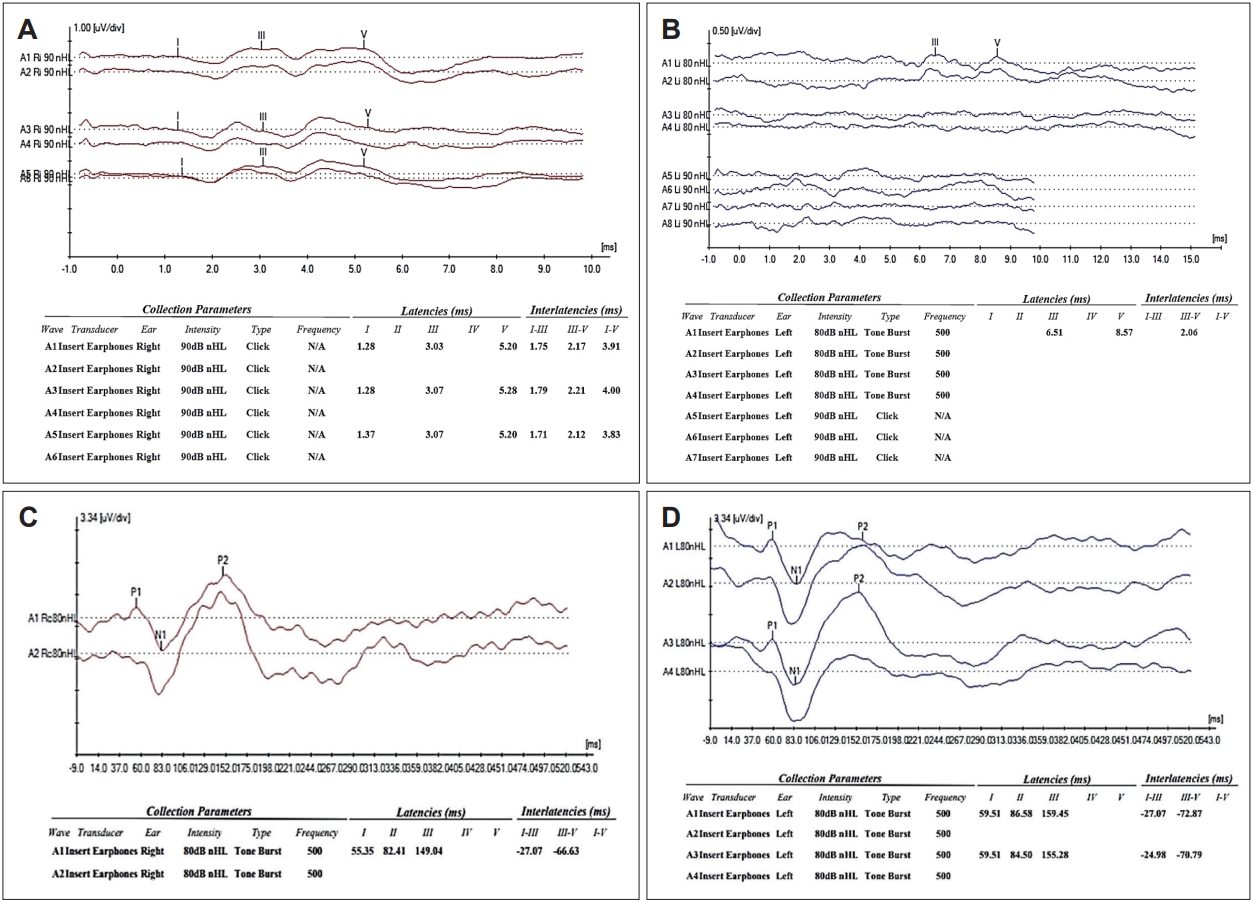
Audiological assessment was once again performed on the patient and results showed similar findings as the first evaluation on pure tone audiometry (Fig. 1B), speech audiometry, immittance results, and OAEs. ABR recording was repeated using both clicks and 500 Hz tone bursts (TB). Results of click ABR showed similar findings as the previous evaluation. During TB ABR recording, the peak V was noted at 8.57 ms in the left ear, indicating a sloping pattern of the audiogram (Fig. 3A and B).
To rule out cortical involvement, auditory late latency responses (ALLR) were recorded using clicks and 500 Hz TB. A calibrated Biologic Navigation Pro system fitted with an ER-3A insert receiver was used for ALLR recording. ALLR recording showed that P1, N1, and P2 peaks were visualized for both the stimulus at normal latencies in the right ear. However, ALLR was not visualized in the left ear for click stimuli. But, for 500 Hz TB stimuli, P1, N1, and P2 peaks were seen within normal limits wherein the latencies of P1 were 59.51 ms, NI was 84.50 ms, and P2 was 153.20 ms, respectively in the left ear (Fig. 3C and D).
Thus, based on the reports of CT scan, ABR, and ALLR of the left ear, the neural basis for the hearing loss can be ruled out. Also, as OAEs are present in the left ear it indicates normal OHC functioning within the cochlea. To confirm the presence of IHC damage/dead, the threshold equalizing noise (TEN) test was done on the patient. In TEN test, dead region in a particular area is indicated by a masked threshold that is at least 10 dB above the actual threshold and 10 dB above the nominal noise. The TEN test results of the present case is shown in Table 2.
Discussion
The present case highlights the utility of test battery approach in knowing the site of lesion with unilateral hearing loss. In the present case, site of lesion in the affected ear (left ear) was the area of concern. Based on the reports of CT scan, ABR, and ALLR of the left ear, the neural basis for the hearing loss was ruled out. Also within the cochlea, OHC function seems to be normal, as shown by the presence of OAEs. Thus, by utilizing the method of exclusion, the possible site of lesion seems to be limited to IHCs/dead regions in the present case. The TEN test was utilized to confirm the presence of dead regions in the present patient. However, the results were inconclusive in the patient, as TEN tests are inefficient to detect dead regions in severe to profound losses unilateral hearing losses; and also any technique for contralateral masking has not been established.
Thus, the present case appears to have selective IHC lesion based on the results of various audiological tests. The patient was earlier diagnosed as having ANSD based on the presence of CM and OAEs in a private hospital. However as the acoustic reflexes were present in the patient and peak V could be visualized during TB ABR recording, the diagnosis of ANSD can be ruled out. Also, there are reports in the literature that show that presence of CM is not exclusive to ANSD but CM can also be noted in patients with sloping hearing losses [5]. In the present patient, OAEs were present at all frequencies, and thus, the present case does not seem to have sloping SNHL. Hence, based on the presence of OAEs and TB ABR with a severe degree of hearing loss in the present case, it can be hypothesized that the site of lesion is limited to IHCs. There are studies in the literature that show that selective IHC damage is likely with normal OHC functioning [6,7]. Thus, the present case seems to be a patient with a rare unilateral SNHL with selective IHC damage and normal OHC functioning.
In conclusion, the importance of the test battery approach for understanding the exact site of lesion in individuals with hearing loss is essential for the accurate diagnosis. In the present case, a rare unilateral SNHL is reported wherein the functioning of OHCs appears to be normal, and there is only selective damage to IHCs which was diagnosed using a test battery approach.