Meta-Analysis Exploring the Effects of Music Training in Cochlear Implant Users by Age
Article information

Abstract
Background and Objectives
The present study aimed to explore meaningful change in the musical performance of cochlear implant (CI) users according to age after receiving music training compared to the other CI users who did not receive any music training and normal hearing (NH) listeners.
Materials and Methods
Article search was conducted from five journal databases. In accordance with PICOS criteria, 29 articles and 15 articles were included for the CI and NH groups, respectively. A total of 44 articles consisting of 407 CI users and 486 NH participants were then analyzed. Using the data gathered from pre- and post-training, meta-analysis was applied by the random-effects model, and then piecewise meta-regression was employed.
Results
CI users with music training showed better performance than those without the training across all ages. The curve change in musical performance when training showed that the CI users was similar to the general pattern of NH performance, indicating that the CI users gained benefits from music training and developed perceptual ability, even though it was not as high as the level of NH counterparts.
Conclusions
This finding supports the benefits of active engagement with music for both CI users and NH listeners, while noting the important role of music as one of the primary aural rehabilitation approaches.
Introduction
With the rapid advancement of technology, most cochlear implant (CI) users today can understand speech by using the device alone, at least in favorable listening conditions. Even though cochlear implantation is one of the most successful approaches for providing useful hearing to many individuals with severe-to-profound hearing loss, the perception and enjoyment of music can be still challenging for these CI users [1,2]. Contemporary researchers have explained that their musical perception ability is poor not only due to reduction in ability to perceive sound, but also limitations of the current devices [3] because the number of distinguishable pitches is interfered with by length of the electrode array, insertion depth, and the number of electrodes [4]. That is, users typically listen to sound altered by focusing more on speech cues rather than musical cues when wearing the CI [5], although musical perception as well as speech perception in noise is very important to them in terms of temporal components used to identify pitch information [3,6].
Indeed, as outcomes for speech reception and language development have successfully improved, the focus of interest has become more diverse regarding the musical perception of CI users [7,8]. CI users are also increasingly hopeful that the benefits of implantation can expand beyond spoken communication to include music participation and enjoyment [9]. Although both music and speech take advantage of acoustic parameter modulation to convey information, the feasibility of musical participation of CI users is complex, in part because music encompasses a diverse continuum from very simple patterns to highly complex combinations [10]. Furthermore, development of musical perception can be affected by several other factors such as age, hearing history, life experiences, and developmental levels in functional areas such as cognition and motor skills that can support musical skills [10]. Thus, many CI users have achieved satisfaction in language comprehension, but still feel limitations when enjoying music while showing large individual variance in accurately recognizing music and its four main components (e.g., pitch, timbre, harmony, and rhythm) [11].
Given the efficacy of musical training offered to CI users based on the literature review, the present study scrutinized the performances of CI users who received music training compared to users who did not receive any music training and their normal hearing (NH) counterparts with typical development. Based on the previous results showing that musical skills develop at different rates depending on age, this study also investigated the effects of age on the performance of both music overall and its main components.
Materials and Methods
The current review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to ensure full transparency and accuracy of findings [12].
Search strategy
The articles were obtained from searching five electronic journal databases: PubMed, CINALH, Web of Science, ScienceDirect, and Scopus from January 18, 2022 to March 29, 2022. According to the Participant, Intervention, Control, Outcome, and Study design (PICOS) inclusion criteria, retrieved articles that contained keywords such as “cochlear implant,” “music training,” one or more of the following music components of “rhythm,” “pitch,” “harmony,” “melody,” and outcomes that related to the keywords “music perception” or “music performance” were further collected and screened (See the lists of keywords in Supplementary Tables 1 and 2 [in the online-only Data Supplement] for CI and NH, respectively).
Inclusion criteria
For the CI group, the study 1) included all ages of CI users from infants to older adults that fit CI unilaterally or bilaterally, 2) used music or at least one or more music components as the main stimuli for the intervention, 3) conducted its investigation by comparing the outcome of intervention to a control group that did not receive any music training or had any past musical experience, 4) had outcome measurements that focused on the improvement of music skills or music-related skills, including the music components, and 5) used a randomized control as a clinical control trial and the pre- and post-study design.
On the other hand, using PICOS criteria specific to the NH population, the participants consisted of NH individuals from all age groups that underwent musical training after being recruited or had musical experience prior to study recruitment. The participants in the control group included NH individuals without any music training or experiences prior to recruitment. The types of study included were randomized control trials, a non-randomized control trial, cohort and clinical trials with control comparison, observational studies, and a study that investigated pre- and post-outcomes after the intervention. The full details on the PICOS criteria of each group are summarized in Supplementary Table 3 (in the online-only Data Supplement).
Quality of study
The significance of the quality of the study was assessed using tools introduced by the National Heart, Lung, and Blood Institute of the National Institutes of Health (NIH) [13]. Each article was assessed using a specific tool for each study design. For this review, three tools were used: Observational Cohort and Cross-Sectional Studies, Controlled Intervention Studies, and Pre- and Post-Studies. The study quality score was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) scale [14] to quantify the quality of the study.
Statistical analysis
The data extracted included mean, mean differences, standard error (SE), and standard deviation (SD). While using the Comprehensive Meta-Analysis (Version 4; Biostat Inc., Englewood, NJ, USA), the analysis combined and quantified the results of individual data to investigate the overall effectiveness of music training on the musical perception skills of both CI users and NH participants. The results obtained from that meta-analysis were further explored using meta-regression. Note that age is an inherent factor that influences the auditory perception development and skill of NH as well as people with hearing loss. However, current publication of meta-analysis was limited only to the linear trend of the data, although improvement in musical performance might not change in its exact linear trend only, as it depends on the age of learning. To overcome this problem and to explore the effects of age on the outcome of music training, we adapted the statistical method from several past studies that proposed dose-response meta-analysis and applied the statistical method introduced by Xu, et al. [15] that is widely used to investigate non-linear trends that depend on the dose given to the participant, while using piecewise regression run using R Software (Ver. 4.2.0, R Core Team, R Foundation for Statistical Computing, Vienna, Austria).
Results
Study selection
In the CI group, a total of 6,929 articles were gathered from the first screening using the specified keywords related to aural rehabilitation using music for CI users. Then, 2,916 duplicates were identified and excluded, leaving 4,013 articles by screening titles and abstracts. Among these, 119 articles were assessed for the next full-article screening after eliminating any irrelevant studies that did not fit the inclusion criteria. A total of 105 articles that did not satisfy PICOS inclusion criteria were further eliminated, leaving 14 eligible articles. These 14 articles, together with 15 articles that were identified in our previous meta-analysis study [11], were included here (Fig. 1A).
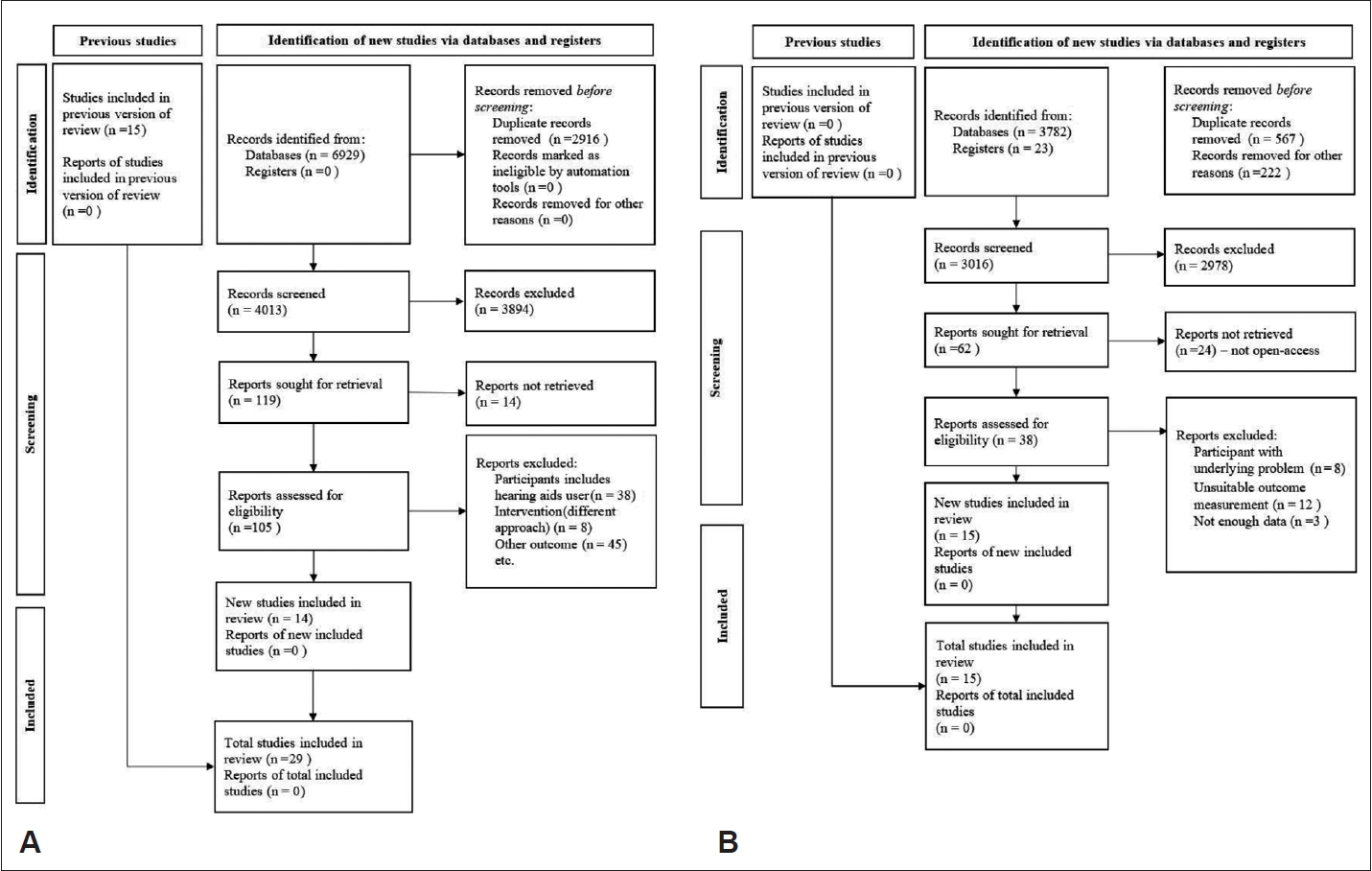
Flow diagram of the PRISMA 2020 version of the article screening process for cochlear implant (A) and normal hearing (B) groups.
For the NH group, 567 duplicates and another 222 records from 3,805 articles were removed before full-article screening, since they did not satisfy the study types and intervention criteria. The remaining 62 articles were reviewed for full-article screening in accordance with the PICOS criteria stated for the NH group. Finally, 15 articles that satisfied all the PICOS criteria listed were included in this study (Fig. 1B).
Study quality
The mean score of the RCT studies for CI group was 11.27 points, while the score obtained for the pre-post study with no control group design was 9 points. They ranged from moderate to high-quality studies in general. Twenty-two controlled intervention studies were assessed using the appropriate tools. Sixteen articles were rated as high-quality [5,16-30], and six of the articles were rated as moderate quality [31-36]. The remaining seven studies were assessed using second tools developed specifically for pre- and post-studies with no-control group design. The result of that assessment revealed 4 studies to be high-quality [37-40] and 3 as moderate quality [41-43].
On the other hand, the articles of NH participants could be divided into two types of study design, namely RCT and controlled intervention. The quality of these RCT studies ranged from moderate to high, with three studies of moderate quality [44-46] and another seven studies classified as high [47-53]. For the controlled intervention studies, 4 studies were classified as high-quality [54-57], and one study was moderate quality [58]. Overall study quality mean was 11.4 for the RCT study, and 11.44 for the controlled studies.
Study characteristics
Data from 407 participants fitted with CI unilaterally (n=246) and bilaterally (n=161) were included in the group, while comparing 486 NH as the control group. The age of the participants ranged between 0 month to 72.7 years old. The implantation age of the participants ranged from 1 year to 9 years for participants aged 0 to 15 years old, and 23 to 31 years for participants aged higher than 15 years old. The mean CI experience of all the participants was 2.52 years (range: 2 to 36 months) for participants aged 0 to 15, and 10.52 years for participants aged more than 15 years old.
Various music training protocols that included different music stimuli, activities, and programs were noted in the articles included. The study used musical instruments as stimuli [21,23,25,29,33,42,43,59,60]. Participants’ abilities to discriminate between each instrument before and after the administration of music training were measured as the main outcome of the study. The stimuli consisted of a wide range of frequencies, including low, middle, and high. Furthermore, the instrument used in the study consisted of several instruments from different instrument families such as piano, cembalo, and an electronic keyboard. Most of the study used an existing famous children’s song, and one study by Yang, et al. [35] used self-composed songs. Two studies [32,38] used a self-developed program that consisted of several tests, including those for timbre, tempo, dynamics, and texture that focused on the development of these skills in infants. Two studies directly measured CI users’ melodic perceptions using a melodic contour identification task [27,42], and two other studies [37,41] focused on rhythm as their main component while pursuing rhythm training. Full-article criteria were summarized in accordance with PICOS strategies in Supplementary Tables 4 and 5 (in the online-only Data Supplement) for the CI and NH groups, respectively.
Publication bias
Even though the funnel plot can be seen as slightly asymmetrical, no significant publication bias was detected in the Egger’s regression results for the CI group (intercept=6.47, SE=1.20, p=1.212) and NH group (intercept=5.34, SE=0.70, p=0.567) (Fig. 2).
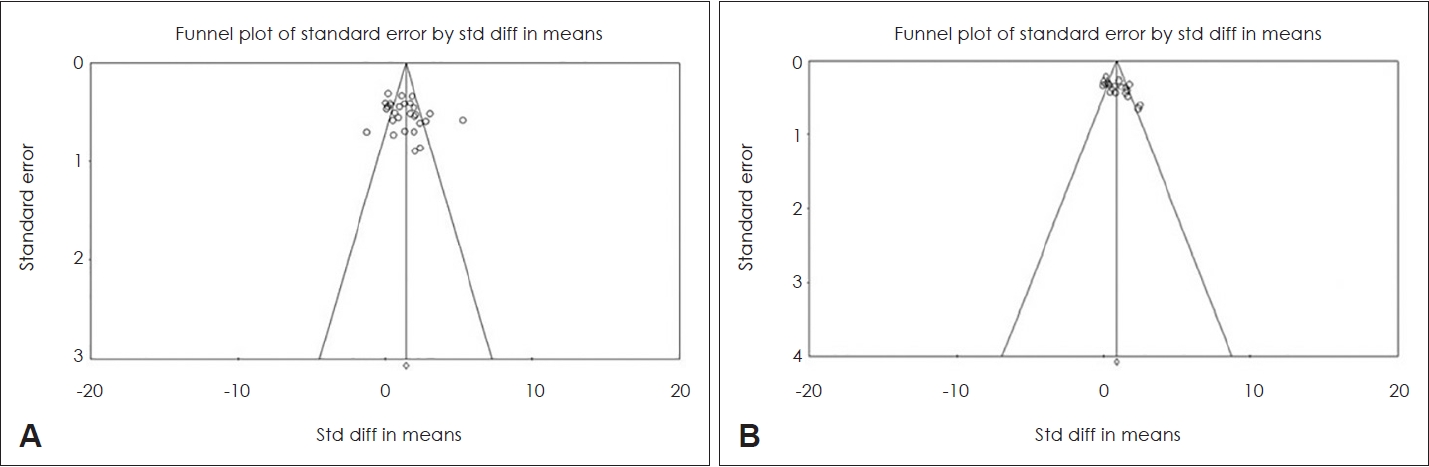
Visualization of publication bias exploration through funnel plot for cochlear implant (A) and normal hearing groups (B).
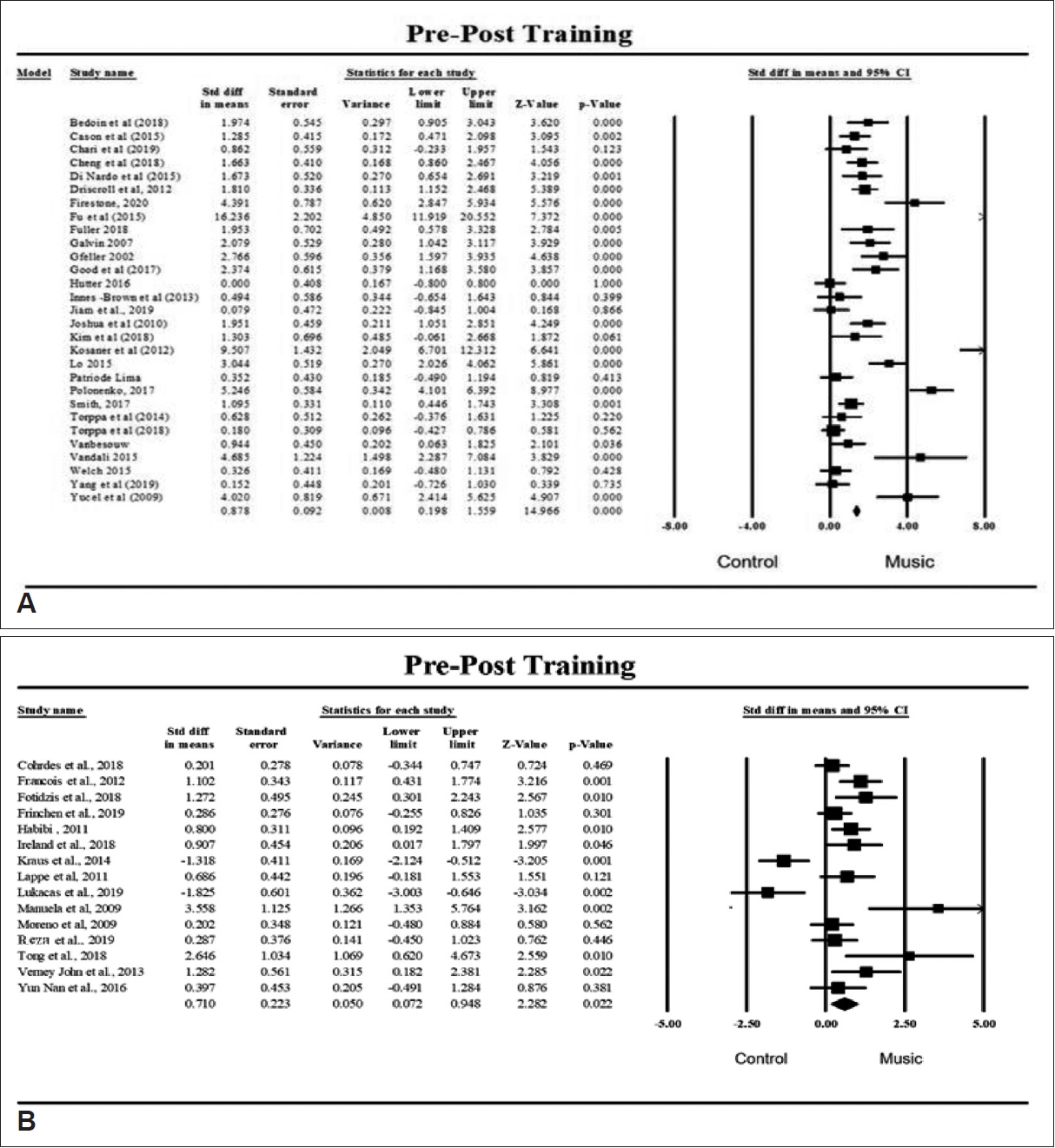
Overall effect of music training
In the pooled analysis, the musical perception was significantly higher after music training for the CI group (standardized mean difference [SMD]=0.88, 95% confidence interval= 0.20 to 1.56, p<0.001) and the NH group (SMD=0.71, 95% confidence interval=0.07 to 0.95, p=0.022) (Fig. 3). Due to moderate heterogeneity between the studies in the CI (I2=52.16, p<0.001) and NH (I2=55.81, p=0.003) groups, we conducted a meta-regression to investigate further the source of heterogeneity and explore the relationship of age to musical performance.
Meta-regression of age contribution to musical performance
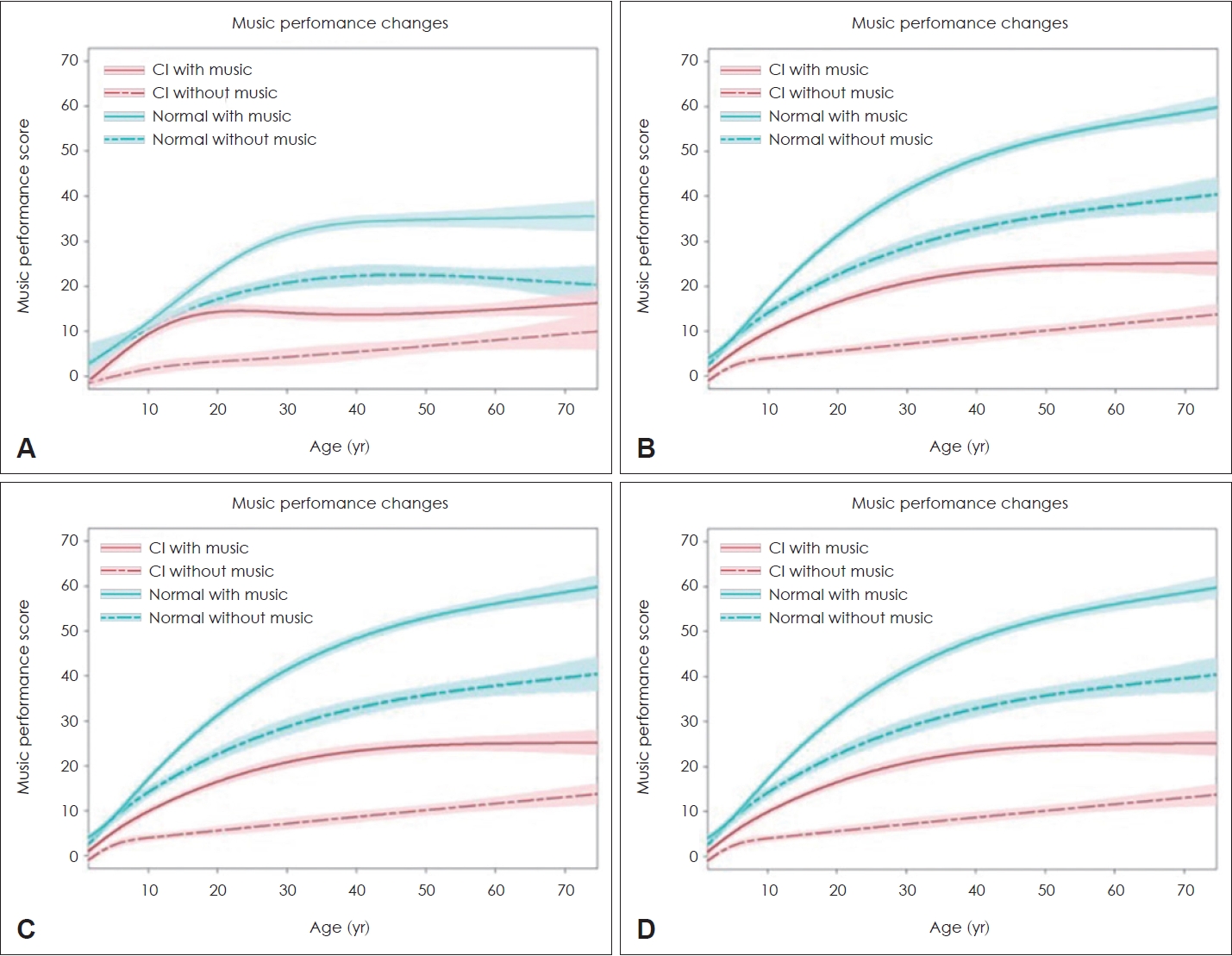
Graphs for CI users’ performance together with NH performance with and without music training are illustrated in Fig. 4.
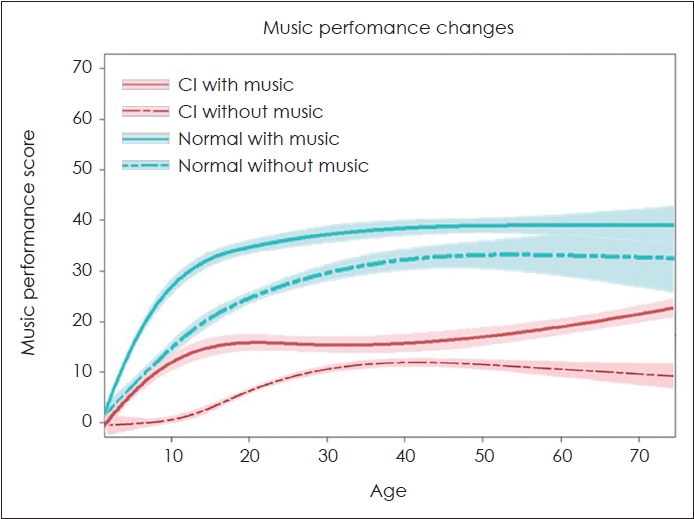
The goodness of fit and 95% confidential interval range (colored area) of meta-regression for cochlear implant (CI) users with (red solid line) or without (red dotted line) training group, together with the normal hearing (NH) group with (blue solid line) and without (blue solid line) music training.
Results for CI users with music training performance revealed a significant increase in performance for all age groups with p-values less than 0.05, especially for participants below 21.13 years in age (coef=12.63). Performance continued to increase for participants aged 21.13 to 54.75 years old (coef=1.71) and for participants aged above 54.75 years (coef=-1.91). This trend also was seen for those without music training where performance was most rapid in the younger age (below 21.53 years old, p<0.001, coef=6.23) compared to slower performance of the participants aged 21.53 to 41.53 (p<0.001, coef=1.41) and older adults aged 41.53 and above (p=0.410, coef=0.87). The performance curve of CI users mimicked the curve of NH individuals, especially in groups that received music training, even though their performance was poorer. The performance of NH showed a significant increment with participants aged below 20.36 years old (p<0.001, coef=12.90), whose performance increased rapidly in comparison with the participants aged 20.36 to 52.79 years old (p<0.001, coef=1.64) and aged above 52.79 years old (p<0.001, coef=6.72).
Meta-regression of age contribution by musical components
The meta-regression results for both the CI and NH groups are summarized in Table 1. The pooled result of meta-regression for each component is illustrated in Fig. 5 for rhythm, pitch, timbre, and harmony.

Meta-regression data for the association of age with musical performance of cochlear implant (CI) and normal hearing (NH) groups with or without music training
The graphs of meta regression (goodness of fit and 95% confidence interval; colored shade) for cochlear implant (CI) and normal hearing (NH) groups for rhythm (A), pitch (B), timbre (C), and harmony (D) performance in relation to age with (solid line) and without (dotted line) music training.
Rhythm
The rhythm performance was affected by the age of CI users. The regression analysis showed that the effect size increased for each age increment with all p-values obtained being lower than 0.001. However, the most rapid increment was seen in the CI users who received music training aged below 14.40 years (coef=12.87). The performance of rhythm for CI users aged 14.40 to 26.00 years old was slightly decreased (coef=-1.28) and increased again after reaching 26.04 years and above (coef=10.02). In contrast, rhythm performance of CI users without any music training did not show any significant performance changes as age increased for participants aged from 14.99 to 24.87 years old (p=0.213, coef=-3.27), and aged above 24.87 years old (p=0.111, coef=6.87). All p-values were found to be greater than 0.05, except for participants aged below 14.99 years old (p=0.111, coef=1.55) that had significant rhythm performance change for this age group.
For the NH group, significant changes were only found for participant at aged 21.53 years and below (p<0.001, coef=12.35) for those with music training and participants below 15.04 years old (p=0.015, coef=0.61) without music training. There were no significant changes in rhythm performance as age increased for participants aged 21.53 to 41.53 years (p=0.158, coef=-4.08) and 41.53 years and older (p=0.388, coef=3.92).
Pitch
The graph for CI users with music training highly fit the current regression model (r2=80.84%). From the curves, the performance changes pre- and post-music training can be seen as being significantly better and higher than those subjects without music training for both the CI and NH groups. A statistically significant p-value was found for all age timepoints. Pitch performance rapidly increased with the increment of age for younger participants below 11.62 years old (p<0.001, coef=5.25, 95% confidence interval=3.27 to 6.79), compared to participants aged between 11.88 and 56.51 (p< 0.001, coef=3.62, 95% confidence interval=2.98 to 7.54) and participants aged above 56.51 (p<0.001, coef=2.30, 95% confidence interval=1.88 to 3.86). However, the pitch performance of CI users without music training was found to be lower than those with music training, with significant changes only seen in participants aged below 11.62 years (p<0.001, coef=4.56). Non-significant p-values for ages 11.62 to 54.72 years (p=0.250, coef=-3.25) and ages above 54.72 years (p=0.33, coef=0.98) indicated that the performance of CI users did not significantly change as age increased.
The NH group also revealed significant improvement as age increased and was especially rapid for participants between 6.81 and 11.33 years old (p<0.001, coef=25.36), followed by those below 6.81 years in age (p=0.003, coef=12.02) and above 11.33 (p<0.001, coef=25.90). The only significant changes were seen in participants aged 6.82 to 18.62 years (coef=2.66, 95% confidence interval=1.03 to 3.53) with a p-value of p<0.001. The performance changes for participants between age 18.62 and 54.72 years (p=0.1522, coef=-1.43, 95% confidence interval=-56.24 to 8.76) and above age 54.72 (p=0.200, coef=0.98, 95% confidence interval=-18.93 to 90.41) were not significant. In other words, pitch performance did not significantly change with age increments starting at 18.62 years.
Timbre
Significant performance changes for NH participants can be seen across all age groups. The steepest slope indicating the most rapid changes were seen for participants aged below 10.25 years (p<0.001, coef=2.56). The performance for the age group 19.21 to 56.7 (p=0.016, coef=1.41) and above 56.7 years (p=0.028, coef=1.08) changed significantly with age for both groups. In contrast, for the NH group without music training, the significant changes are only seen for the participants aged below 19.21 years (p<0.001, coef=2.71). Comparison with the NH group also revealed that CI users’ performance was lower and slower than for those with NH who received music training. However, the meta-regression model investigating the performance of timbre to age did fit properly with the current model with both r2 value for groups with music (r2=27.77%) and without music (r2=12.78%). Thus, an appropriate conclusion cannot be derived from the results obtained.
Harmony
The CI users’ harmony performance could not be properly derived from the result, as the data did not fit the current regression model. The r2 values were indicated as a poorly fitted graph (music=0.6%, without music=0.0%). In other words, the regression model was not able to explain the data of harmony performance in relation to age. On top of that, all pvalues of the graph yielded significant changes for harmony performance as age increased from below 8.23 years (p=0.231, coef=0.98), 8.23 to 14.52 years (p=0.980, coef=0.51), 14.54 to 45.31 years (p=0.324, coef=0.32) and above 45.31 years (p=1.412, coef=2.11). For the group without music training, insignificant changes were also seen in the age group below 15.21 years (p=0.89, coef=1.32), 15.21 to 26.90 years (p=1.080, coef=0.96) and 26.90 years old and above (p=1.120, coef=1.01). From visual inspection, the harmony performance of the CI group was lower than for the normal group. However, the graph fit of relation was low (with music r2=25.66, without music r2=11.28%) to indicate that only 26% and 11.28% of the data were explained by the fitted graph, and proper results thus could not be concluded for this group.
Discussion
How do CI users’ music performance changes with music training compared to the NH counterparts?
Musical development is a complex, dynamic, and non-linear process that is influenced by a wide range of interrelated factors, including maturation of the brain and body, cultural practices, values, and quality of engagement with music via learning experiences [61]. The current study found that the curve of music performance of CI with musically trained participants closely mimicked the curve of NH individuals with music training, thereby suggesting that CI users might benefit from music training. The musical performance of CI users was seen to rapidly increase for CI users aged below 15 years old, similar to the NH individuals. Past studies have revealed that musicians that started learning music at a younger age (below 7 years old) showed better musical skills compared to musicians that started at a later age [62]. Furthermore, for musical expertise, musicians that started training at a younger age also have better skills than musicians who started training at a later age, even though both groups have the same level of experience [63]. Even though the changes in musical performance are not as rapid as for CI users under 15 years old, CI users aged above 15 years can also have improved performance with music training like the NH participants.
The researchers agreed that, unlike speech that has a “critical period,” musical skills have a “sensitive window” during which both musical perception and skills rapidly develop, and certain musical skills such as perfect pitch can only be learned during this period [64]. From our results, note that this sensitive window can be seen happening before 15 years of age for overall musical skills. Although musical skill can also be seen as increasing after 15 years old, it does not increase as rapidly as those below this age and yet will develop steadily as age increases. Bailey and Penhune [65] agreed that the development of musical skills also depends on training duration, exposure to music, brain plasticity, and individual motivation for learning music, which means that musical skills can indeed be learned at any age.
A comparison in performance between the CI and NH groups revealed that the performance of NH group was better even at the age of 0 years because for NH fetuses, the auditory system becomes functional at around 25 weeks’ gestation [66]. Infants with NH seem to be born with innate musical abilities. Even small infants can detect pitch, timbre, and duration of sounds, recognize familiar melodic and rhythmic patterns, prefer consonant over dissonant music, and prefer singing over speech [67]. This development, however, is limited or restricted for most congenital hearing loss, which explains why NH infants perform better than those with CI, even when they are implanted at an early age [67,68].
Does each music component have its own “sensitive window”?
An idea of the “sensitive window” gained the most widespread attention through the results of several studies showing that musical skill is greater in individuals who were exposed to music before ages 11–13 [64-68]. As expected, each component’s sensitive window might be different from the other in our analysis. Studies have shown that rhythm compared to other components is probably the easiest attribute cap reached accurately by CI listeners [69,70]. The current study revealed that the rhythm performance of CI aged below 10 years showed rapid improvement as age increases, which was in line with the finding by Ireland, et al. [49] stating that children who received music training before 7 years old outperformed children who started later for simple rhythm/melody discrimination, but not complex rhythm synchronization. In addition, Torppa, et al. [43] found that adults also can learn rhythm, even when trained at a later age. However, it is important that the increment of rhythm-related skills for adults was not as rapid as for children below 15 years old, with children below 8 years old showing the highest improvement in their rhythm skills.
Even though pitch is one of the elements that is difficult to convey to CI users, many previous studies have shown that pitch skill can indeed be improved with music training. Our analysis showed that pitch skills of CI children also develop rapidly at ages below 12 years, similar to the NH group that shows the most rapid pitch performance changes at below 15 years. This result supports the findings from Yvert, et al. [71] in that the brain responses (P1 component), which are responsible for the perception of pitch, are clearly present in the youngest children, increase somewhat in amplitude with increasing age, and reach a maximum at around 9 years of age. Another study done by Lappe, et al. [58] found that N1 and P2, which likely reflect activation of the secondary auditory cortical area and may reflect communication between cortical areas, are absent in the youngest ages, increase dramatically after age 6, reach a maximum around 10 to 12 years of age, and decrease thereafter while still remaining prominent into adulthood [72].
Due to the small number of articles discussing timbre and harmony performance, appropriate conclusions could not be extracted from the present results. Nevertheless, timbre is considered an essential attribute of music that also helps in the differentiation of speakers’ voices and subsequently contributes to understanding speech [73]. The difference between the pre- and post- results for timbre performance, even though of a small effect size, has been found to be statistically significant in our previous study [11]. However, the extent to which music training can help in developing timbre perception skills for CI users has not yet been well investigated, especially for the larger population. The performance changes in harmony known as complex attributes of music also could not be fully explored in the current study. However, the previous research found that 7-year-old children with NH could detect “out ofkey” and “out-of-harmony” changes much more easily than “within-harmony changes,” whereas 5-year-olds reliably detected only the “out-of-key changes” [74]. These findings suggest that 5-year-olds have implicit knowledge of key membership, but not of implied harmony, whereas 7-year-olds, like adults, have implicit knowledge of both aspects of music structure [74]. This knowledge marks harmony skills in children that can reach adult skill levels at age 7 years [75]. However, keep in mind that more study on both timbre and harmony skills development for CI users’ is needed to explore further the development of these attributes not only in children, but also to see whether harmony can also be learned by young adults and older adults.
Clinical implications and limitations of study
The benefits of music training may be accessible to every age at different rates, and not only to the younger population. It seems to be important that clinicians provide both children and adults an equal opportunity to improve their listening skills through music training. The current protocol for music training may not be able to replace traditional intervention methods for the hearing impaired; however, with systematic and scientific-based development of the music training protocol as an auditory training approach together with the traditional approach, active engagement with music may provide a valuable proportion of the aural rehabilitation program.
Unfortunately, due to a lack of uniformed music protocol, the duration of music training administered to the participants could not be controlled in this review and meta-analysis. We assume that duration of music training or the exposure to music might affect performance skill development or improvement of participants. In addition, data of pre- vs. post-lingually implanted CI users were not separated in this study, even though we recognize that the performances of the two populations were significantly different due to the natural hearing experiences of post-lingual CI users. Thus, the analysis should be run separately as implantation times in the following study. Also, with more new publications, more studies can be included to explore further the development of timbre and harmony to provide significant and meaningful insights.
Conclusion
The present study provides evidence of the benefits of active engagement with music throughout the lifespan of CI users. The effect of music training can be seen in all age groups, suggesting that all age groups experience positive effects from music training but at different rates. In early childhood, especially those before aged 12 to 15 years, development of music perception and skill seems to be the most rapid, which subsequently improves spatial reasoning, motor coordination, literacy, and self-perception. Older adults were seen to have the lowest improvement after music training compared to young adults and children. While the performance of CI users falls short of NH levels, we conclude that music training can indeed help improve the musical performance of CI recipients, and music training should be introduced earlier, especially for CI users aged between 0 to 15 years old, to achieve the maximum benefit from the training.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.7874/jao.2023.00087.
Supplementary Table 1.
Full electronic search strategies of the cochlear implant group for all database used in the study
Supplementary Table 2.
Full electronic search strategies of normal hearing group for all database used in the study
Supplementary Table 3.
The PICOS criteria of the present study for cochlear implant (CI) and normal hearing (NH) groups
Supplementary Table 4.
A table summary of included studies according to the PICOS criteria for cochlear implant group
Supplementary Table 5.
A table summary of included studies according to the PICOS criteria for normal hearing group
Acknowledgments
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF2022S1A5C2A03091539). Also, this study is a portion of the master’s thesis work for the first author.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: all authors. Data curation: Nor Farawaheeda Ab Shukor, Woojae Han. Formal analysis: Nor Farawaheeda Ab Shukor, Woojae Han. Funding acquisition: Woojae Han. Methodology: Nor Farawaheeda Ab Shukor, Woojae Han. Project administration: Young Joon Seo, Woojae Han. Visualization: Nor Farawaheeda Ab Shukor. Writing—original draft: Nor Farawaheeda Ab Shukor. Writing—review & editing: all authors. Approval of final manuscript: all authors.