A Case with the Bilateral Narrow Bony Cochlear Nerve Canals Associated with Near Normal Hearing Thresholds
Article information
Abstract
The narrow bony cochlear nerve canal in high resolution temporal bone computed tomography is frequently found in patients of congenital sensorineural hearing loss. But this bony structural anomaly could not conclude the functional outcome of cochlear nerve. Here, we present a case of a 14-month-old girl having bilateral narrow bony cochlear nerve canals. In magnetic resonance imaging, both the cochlear nerves were identified to be intact. Moreover, acoustic brainstem response threshold and auditory steady state response revealed nearly normal hearing thresholds. Therefore, we suggest that the narrow bony cochlear nerve canal itself does not necessarily indicate a substantial degree of hearing loss.
Introduction
With advancement of a radiologic imaging technique, more information can be obtained from the imaging and it would give a hand to diagnosis and decision making for treatment. High resolution temporal bone computed tomography (TBCT) and internal auditory canal magnetic resonance image (IAC MRI) provide detailed images of inner ear and cochleovestibular nerve. High resolution TBCT is a tool commonly used to evaluate structures of the middle ear and inner ear when the structural deformities or anomalies are clinically suspected. Recently, narrow bony cochlear nerve canal (BCNC) is identified and attracts a lot of attention.1,2) The BCNC is the short canal between the base of the cochlear modiolus and the fundus of the internal auditory canal (IAC) carrying the cochlear nerve fibers from spiral ganglion to cochlear nucleus.3) Narrow BCNC is considered when the width is less than 1.4 mm to 1.5 mm.3)
Some sensorineural hearing loss (SNHL) patients show narrow BCNC or narrow IAC in TBCT or IAC MRI.1,4,5) Furthermore, both the BCNC and IAC are frequently narrower in the affected side of unilateral SNHL.6,7) In other way, cochlear nerve deficiency (CND) is shown in the substantial proportion of narrow BCNC cases.8,9) Therefore, it can be deduced that the narrow BCNC as detected by the TBCT would play some role in the SNHL.
However, it is noteworthy that the intact cochlear nerve is frequently visualized by IAC MRI in the bilateral narrow BCNC cases5,10) contradicting the previous studies that the CND coincides with the narrow BCNC.8,9,11) Therefore, we cannot conclude that the absence or hypoplasia of cochlear nerve necessarily accompanies the narrow BCNC especially in bilateral cases. However, there is a recent case report for the narrow BCNC not accompanied by profound hearing loss.12) In the report, auditory brainstem response (ABR) was not detected even though only mild hearing loss was documented in pure tone audiometry (PTA).12) It shows that narrow BCNC does not always lead to profoundly elevated pure tone thresholds. However, the absence of ABR responses implied the broken integrity of the cochlear nerve, which was in line with the CND shown in IAC MRI.
Here, we report a case with the bilateral narrow BCNC but with the intact cochlear nerve and nearly normal ABR thresholds.
Case Report
A female newborn was referred to department of otorhinolaryngology in a tertiary hospital for evaluation of congenital both ear pits. She had intra-partum and post-partum medical problems such as low birth weight, intrauterine growth retardation, ventriculomegaly, fetal hydronephrosis, umbilical hernia, and craniofacial anomaly.
On physical examination, she had cup ear deformities, depressed helix, and both preauricular fistulae in both auricles. But her both tympanic membranes were normal. In newborn hearing screening automated acoustic brainstem response (AABR) performed with AccuScreen (GN Otometrics, Copenhagen, Denmark), both ear were reported as "refer". Then, acoustic brainstem response threshold (ABRT) and auditory steady state response (ASSR) were performed with Navigator PRO system and MASTER system (Bio-logic, San Carlos, CA, USA) and they were checked at the age of 2 months and the results were that right and left ABRT was 25 dB and 30 dB, respectively and right and left ASSR were 25 dB and 30 dB in average, respectively (Fig. 1).
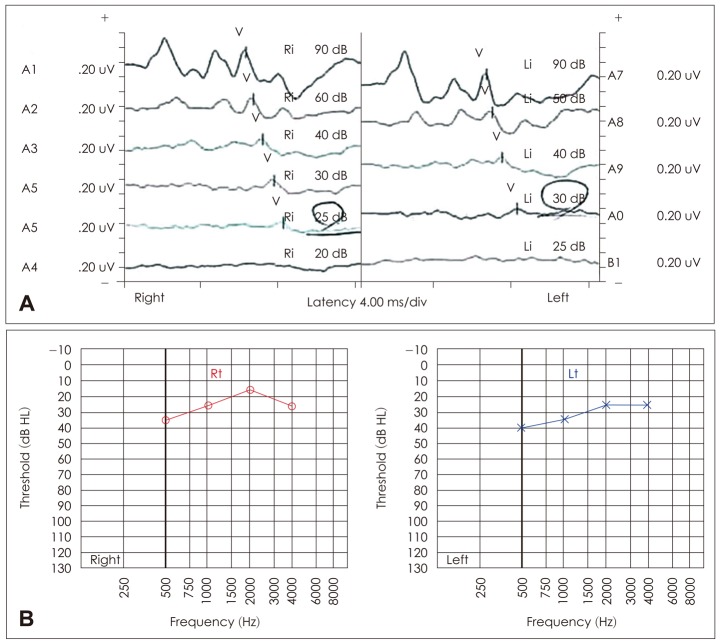
Acoustic brainstem response threshold (ABRT) and auditory steady state response (ASSR). A: ABRT illustrated right 25 dB HL and left 30 dB HL. B: ASSR illustrated right 25 dB HL and left 30 dB HL.
The 0.7 mm thickness high resolution TBCT performed with Philips Brilliance computed tomography 64-channel scanner (Philips Medical Systems, Cleveland, OH, USA) showed the significantly narrow BCNC (Fig. 2) in which the right and left diameters were 0.6 mm and 0.9 mm, respectively (the right 0.6 mm and left 0.9 mm diameters have accuracy 42.9% and 64.3% in the 0.7 mm thickness images but both diameters are less than 1.4 mm, the cutoff diameter of BC-NC, in 100% accuracy).
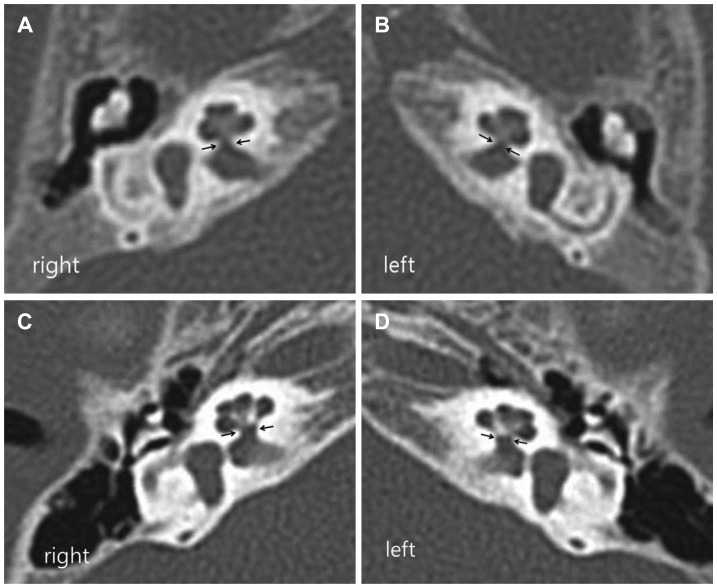
Axial section of TBCT of the case patient and the control patient who is a 8 month-old girl with congenital bilateral sensorineural hearing loss and normal bony cochlear nerve canal width (field of view: 100×100 mm, window width: 4000, window level: 300, thickness: 0.7 mm). A: The width of right BCNC (between black arrows) was 0.6 mm in the case patient. B: The width of left BCNC was 0.9 mm in the case patient. C: The width of right BCNC was 1.7 mm in the control patient. D: The width of left BCNC was 1.6 mm in the control patient. TBCT: temporal bone computed tomography, BCNC: bony cochlear nerve canal.
At the age of 14 months, distortion product otoacoustic emission (DPOAE) was performed with ILO (Otodynamics, Hatfield, UK) and IAC MRI was performed with a Philips 3.0 T Achieva (Philips Medical Systems, Best, the Netherlands). There were no response of DPOAE in right ear and small response of DPOAE only in left ear. This time she had effusion on right tympanic membrane.
The cochlear nerve in high resolution T2 weighted IAC MRI and constructive inference in steady state (CISS) MRI revealed an intact cochlear nerve in both sides (Fig. 3). No vestibular symptom, such as recurrent vomiting, abnormal gait or fall-down, and spontaneous nystagmus have been reported.

Parasagittal constructive interference in steady state MRI (field of view: 160×160 mm, window width: 600, window level: 280, thickness: 0.6 mm). Parasagittal CISS image was achieved by perpendicular plane to the internal auditory canal in both coronal and axial images. A: Right cochlear nerve entered into cochlear basal turn. B: Right cochlear nerve was identified in IAC. C: Left cochlear nerve entered into cochlear basal turn. D: Left cochlear nerve was identified in IAC. CN: cochlear nerve, FN: facial nerve, SVN: superior vestibular nerve, IVN: inferior vestibular ner-ve, CISS: constructive inference in steady state, IAC: internal auditory canal.
Discussion
Congenital sensorineural hearing loss is associated with bony abnormalities of the inner ear visible on CT in only 20% of cases.13,14) Up to recently, narrow BCNC has been considered one of the abnormalities which might easily explain the CND and resultantly, SNHL. However, narrow BCNC does not necessarily associate morphological aplasia or hypoplasia of cochlear nerve in IAC MRI and CISS images.5,10) Most of the narrow BCNC cases without CND have also been accompanied by severe or profound hearing thresholds. Further, it has been recently reported that the narrow BCNC is not always accompanied by significant SNHL and sometimes can be associated with only subtle hearing loss even under the invisible cochlear nerve by MRI and poor ABR responses.12) However, the narrow BCNC case without both CND and hearing loss has rarely been reported in the literature. In this study, we clearly present a narrow BCNC case where there is neither significant hearing loss nor the presence of CND, showing that we can suspect this anomaly even under near normal hearing status.
In our study, the patient underwent AABR one time and had "REFER" sign in both ears. At that time, both tympanic membranes were free of pathologic findings. AABR have been conducted in newborn hearing screening with high referring rate 6.5%.15) Considering the high referring rate of AABR, near normal results of ABRT and ASSR shows that AABR was false positive. The following DPOAE in 14-month-old revealed no response on the right ear. It was also false positive result of DPOAE since the right tympanic membrane showed effusion under the otoscope examination. Therefore, the near normal electrophysiologic audiometric results in this case suggested that we should include narrow BCNC as one of differential diagnosis even in subtle to mild SNHL.
The narrower BCNC width 0.6 mm on right ear of the case seemed to oppose the better ABRT and ASSR result 25 dB HL on right ear. But the cross section of BCNC must not have an exact circle. It can be a ovoid or irregular. With the variety of the sectional shape of BCNC, considering accuracy of the BCNC width under 0.7 mm thickness TBCT, 0.6 mm and 0.9 mm on the axial-plane images could not conclude the 3-dimentional size difference. In other words, the size less than 1.4 mm under the 0.7 mm thickness axial-plane images can be confirmed with 100% accuracy but the size difference less than 1.4 mm cannot be concluded. In the case, the right BCNC might not be smaller than the left one.
The limitation of this case report is that only electrophysiological hearing tests were conducted such as AABR, ABRT, ASSR and DPOAE without PTA and speech audiometry (SA). So far, we could verify her hearing level with only electrophysiologic tests. The direct hearing tests, such as PTA and SA, are required to evaluate her hearing in near future.
There were many reports about morphological integrity of cochlear nerve in narrow BCNC. Also there was a few reports about mild hearing loss in narrow the BCNC. Given this, this is the report suggesting that a phenotypic spectrum of the narrow BCNC may range to the intact cochlear nerve and the near normal auditory threshold. The narrow BCNC should also be included as a differential diagnosis when a subtle hearing loss is encountered.
Acknowledgments
This study was supported by the Seoul National University Bundang Hospital research fund [No. 04-2010-003 (to Choi, B.Y)].