Combination Therapy with Systemic Steroids, an Antiviral Agent, Anticoagulants, and Stellate Ganglion Block for Treatment of Sudden Sensorineural Hearing Loss
Article information
Abstract
Background and Objectives
Sudden sensorineural hearing loss (SSNHL) is commonly defined as a loss of at least 30 dB in three contiguous frequencies occurring within 3 days. Systemic steroid administration has become the most widely accepted treatment option for SSNHL. Since viral infection and vascular compromise are considered specific causes of SSNHL, antiviral agents, anticoagulants, and stellate ganglion block have been used for its treatment, although the evidence of their effectiveness is weak. The present study evaluated the hearing recovery rate in the combination therapy group (systemic steroids, antiviral agent, anticoagulants, and stellate ganglion block) in comparison with patients treated with systemic steroids alone.
Subjects and Methods
A total of 85 patients diagnosed with SSNHL were treated with combination therapy (group A, 46 patients) or systemic steroids only (group B, 39 patients). Hearing improvement was defined as a hearing gain of more than slight improvement using Siegel's criteria. All patients were treated with a 10-day course of systemic steroids (10-mg dexamethasone for 5 days, followed by tapering for 5 days). Acyclovir, heparin, and stellate ganglion block were included in the group A treatment regimen.
Results
The overall rate of hearing improvement was 60.9% (28/46 patients) in group A, which was significantly higher than that (38.5%, 15/39 patients) in group B. The distribution of prognostic factors was not significantly different between the two groups with the exception of the degree of initial hearing loss, which was more severe in group A. Upon analysis according to prognostic factors, group A showed a better hearing improvement recovery rate than group B in patients with hearing loss >70 dB, age >41 years, dizziness, and early treatment (<1 week).
Conclusions
Thus SSNHL patients treated with combination therapy have a higher likelihood of hearing improvement than those treated with systemic steroids alone.
Introduction
Sudden sensorineural hearing loss (SSNHL) is commonly defined as a loss of at least 30 dB in three contiguous frequencies occurring within 3 days.1) Lack of knowledge of the specific causes of idiopathic SSNHL limits our ability to implement effective treatment. Although it is possible that a number of different pathological processes result in sudden hearing loss, it is widely believed that viral infection and vascular occlusion account for the majority of these cases.2-4) Systemic steroid administration is the most widely accepted treatment option for SSNHL.5) Since viral infection and vascular compromise are considered specific causes of SSNHL, antiviral agents, anticoagulants, and stellate ganglion block have been used for its treatment, although the evidence of their effectiveness is weak.2-4,6)
In our hospital, one author used a combination therapy consisting of systemic steroids, an antiviral agent, anticoagulants, and stellate ganglion block for the treatment of SSNHL, while two authors employed systemic steroids only to determine whether there is a difference in hearing recovery rate between the two treatment options.
The present study evaluated the hearing recovery rate in the combination therapy group (systemic steroids, an antiviral agent, anticoagulants, and stellate ganglion block) in comparison with the group treated with systemic steroids alone.
Subjects and Methods
Clinical records of subjects with unilateral SSNHL were retrospectively reviewed. A total of 85 patients diagnosed with SSNHL were treated with either combination therapy (group A, 46 patients) or systemic steroids only (group B, 39 patients). The study population consisted of 43 females and 42 males ranging in age from 14 to 77 years, with a mean age of 49.2 years. The left ear was involved in 39 patients and the right in 46. The distribution of sex and age was not different between the two groups.
All patients were treated with a 10-day course of systemic steroids (10 mg of dexamethasone for 5 days, followed by tapering for 5 days). The treatment regimen of group A included acyclovir (250 mg, 3 times daily, 5 days), heparin (low molecular weight heparin 10000 U daily, 10 days), and stellate ganglion block (daily by anesthesiologist, 5-10 days). Auditory function was determined by pure tone audiometry, and mean hearing levels were expressed as the average of hearing thresholds at 500, 1000, 2000, and 3000 Hz. Auditory measurements were performed before and 2 months after treatment using Siegel's hearing improvement criteria (Table 1). Hearing improvement was defined as a hearing gain of more than slight improvement using Siegel's criteria.
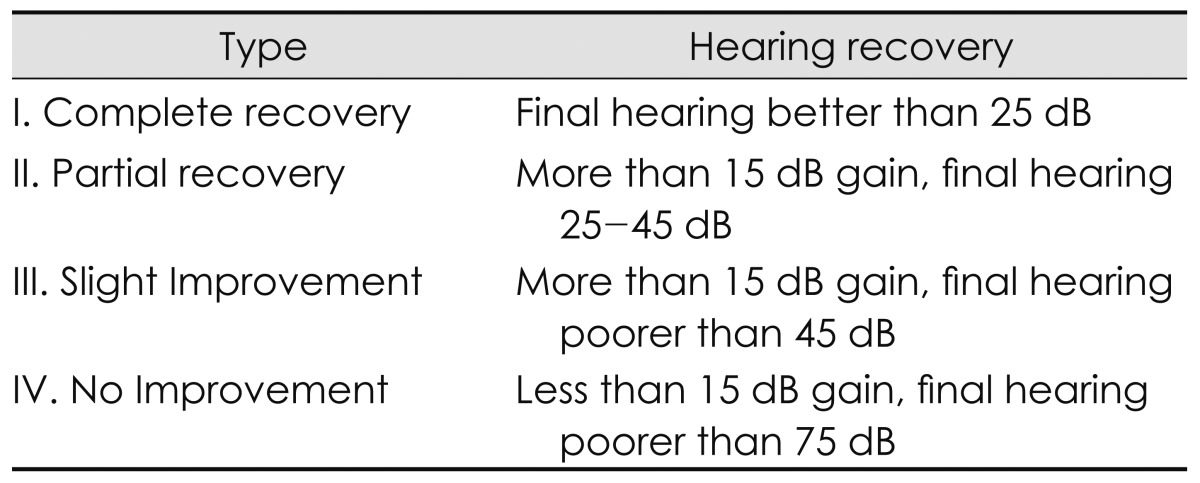
Siegel's hearing recovery criteria
The following prognostic factors were taken into consideration in the analysis of hearing recovery rates: 1) initial hearing level (>70 dB HL), 2) audiogram shape (ascending, descending, and flat type), 3) treatment onset (within 7 days), 4) age (>40 years), and 5) presence of dizziness. Statistical evaluations were performed using the chi-square test, Fisher's exact test, and logistic regression.
Results
The overall rate of hearing improvement was 60.9% (28/46 patients) in group A, which was significantly higher than that (38.5%, 15/39 patients) in group B (p=0.039, χ2 test)(Fig. 1). Group A included nine patients (19.6%) with complete hearing recovery, seven (15.2%) with partial recovery, and 12 (26.1%) with slight improvement. group B included 10 patients (25.6%) with complete hearing recovery, three (7.7%) with partial recovery, and two (5.1%) with slight improvement (Fig. 1).

Hearing recovery rate after combined therapy (group A) and systemic steroids only (group B). Improvement=complete recovery+partial recovery+slight improvement. *p<0.05, χ2 test.
The distribution of prognostic factors was not significantly different between the two groups, with the exception of degree of initial hearing loss, which was more severe in group A (Fig. 2).
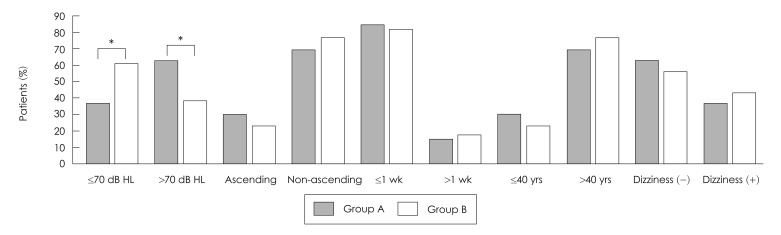
The distributions of prognostic factors were not significantly different between groups A and B, with the exception of degree of initial hearing loss, which was more severe in group A. *p<0.05, χ2 test.
Hearing improvement was analyzed according to the prognostic factors, and the results indicated a better recovery rate in group A compared to group B among patients with hearing loss >70 dB, age >41 years, dizziness, and early start of treatment (<1 week)(p<0.05, χ2 test, Fisher's exact test)(Table 2)(Fig. 3).

Hearing recovery rate according to prognostic factors in groups A and B
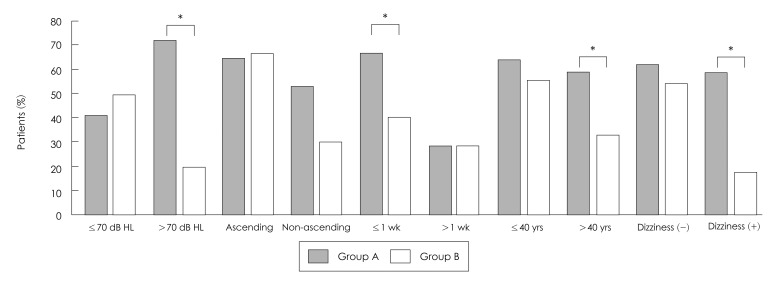
Hearing recovery rate according to prognostic factors in groups A and B. *p<0.05, χ2 test, Fisher's exact test.
Multivariate analysis of potential prognostic factors, including treatment option (group A or B), indicated a significant association between an ascending audiogram shape and good clinical outcome. The level of hearing loss, the pres ence of dizziness, delay of treatment, age >40 years, and treatment options showed no associations with hearing recovery (Table 3).

Multivariate analysis of the significant prognostic factors
Discussion
The current standard treatment for SSNHL is a tapered course of systemic steroids.7) However, data to support this recommendation are limited. A 2006 Cochrane database review concluded that the value of steroids in the treatment of SSNHL remains unclear.8) The mechanism of action of steroids in the inner ear is incompletely understood. The actions attributed to steroids in the inner ear include ion homeostasis, antioxidant activity, inhibition of apoptosis, downregulation of local proinflammatory cytokines, and promotion of cochlear blood flow.5)
The potential success of antiviral medication for treatment of SSNHL is based on the suggestion that many cases of such hearing impairment have a viral etiology.3) Herpes virus may be involved in the etiology of SSNHL by one of several mechanisms, including labyrinthitis secondary to viremia, labyrinthitis or neuritis secondary to meningitis, cranial neuropathy, reactivation of a latent ganglion cell infection, or alteration of the immune response.9) It is possible that the viral damage to the ear is completed within a relatively short time and that inflammatory and other effects of the virus are most effectively treated thereafter with steroids.3) This may explain the observed better recovery rate in group A than group B among patients treated within 1 week in the present study.
The use of heparin and stellate ganglion block is based on the suggestion that impairments in microcirculation of the inner ear may be involved in the pathophysiology of SSNHL.2,4,6) The blood flow disturbance theory, including thromboembolism or vasospasm, has been proposed based on the etiology of SSNHL, because the blood supply within the inner ear is its termination and intraosseous position and symptoms of SSNHL develop abruptly.10,11) Heparin as a treatment for SSNHL was described by Fisch, et al.2) and it has an anticoagulant effect on intracranial blood vessels. However, Mattox and Simmons12) reported no significant difference between patients with and without general heparin therapy. Since the introduction of low-molecular-weight heparin in the early 1990s, its use and indications have been greatly expanded.13) Low-molecular-weight heparin can prevent venous thrombosis and shows greatly reduced side reactions compared with general heparin. Yue, et al.4) suggested that hearing improvement is significantly greater in patients treated with low-molecular weight heparin than in those treated with the commonly used therapeutic regimen alone.
Stellate ganglion block induces an increased blood supply via sympathetic blockade and vasodilation.14) The eventual involvement of internal ear circulatory disturbance causes metabolic disturbance of the inner ear cells, decreases in oxidation of metabolic substrates, and edema, resulting in irreversible changes. The resorption of edema is promoted by arterial relaxation from sympathetic blockade.6,15) Takinami15) reported that stellate ganglion block favorably affected outcomes in patients with unilateral SSNHL given a prior or concomitant course of systemic corticosteroids.
The combination therapy showed a beneficial effect in the present study; however, the analysis was performed in a retrospective manner. Especially in patients with poor prognosis, the combined therapy resulted in a higher recovery rate than steroids alone, although the complete recovery rate was not different between the two treatment methods. The efficacy of combination therapy cannot be established definitively in a retrospective analysis with a small sample size. Therefore, our results indicate only a trend toward a beneficial effect of combination therapy as a component of SSNHL treatment.
Conclusion
The results of this study suggest that SSNHL patients treated with the combination therapy have a higher likelihood of hearing improvement than those treated with systemic steroids alone.