Introduction
Spontaneous upbeat nystagmus (UBN), also known as primary position UBN, is a rare type of acquired nystagmus, usually attributed to disorders involving central oculomotor pathways [1]. Anecdotally, it has also been associated to inner ear pathologies [2], besides vestibular migraine in which peripheral and central mechanisms could be implicated [3]. Benign paroxysmal positional vertigo (BPPV) is considered the most common labyrinthine disease where displaced otoconia usually settle the posterior semicircular canal (PSC) due to its undermost position. Diagnostic maneuvers should elicit paroxysmal UBN with ipsilesional torsional components (i.e. the top pole of the eyes beating toward the undermost ear) due to resulting ampullofugal excitatory flows within the affected PSC [1]. Conversely, in rare cases of anterior semicircular canal (ASC) involvement, positionings are expected to evoke downbeat nystagmus (DBN) due to an ampullofugal shift of free-floating particles exciting ASC afferents [1,4]. Nowadays, thanks to the accessibility of the video-head impulse test (Video-HIT) and vestibular-evoked myogenic potentials (VEMPs) for clinical purposes, a precise measurement of the activity of each inner ear sensor is easily provided.
Case Report
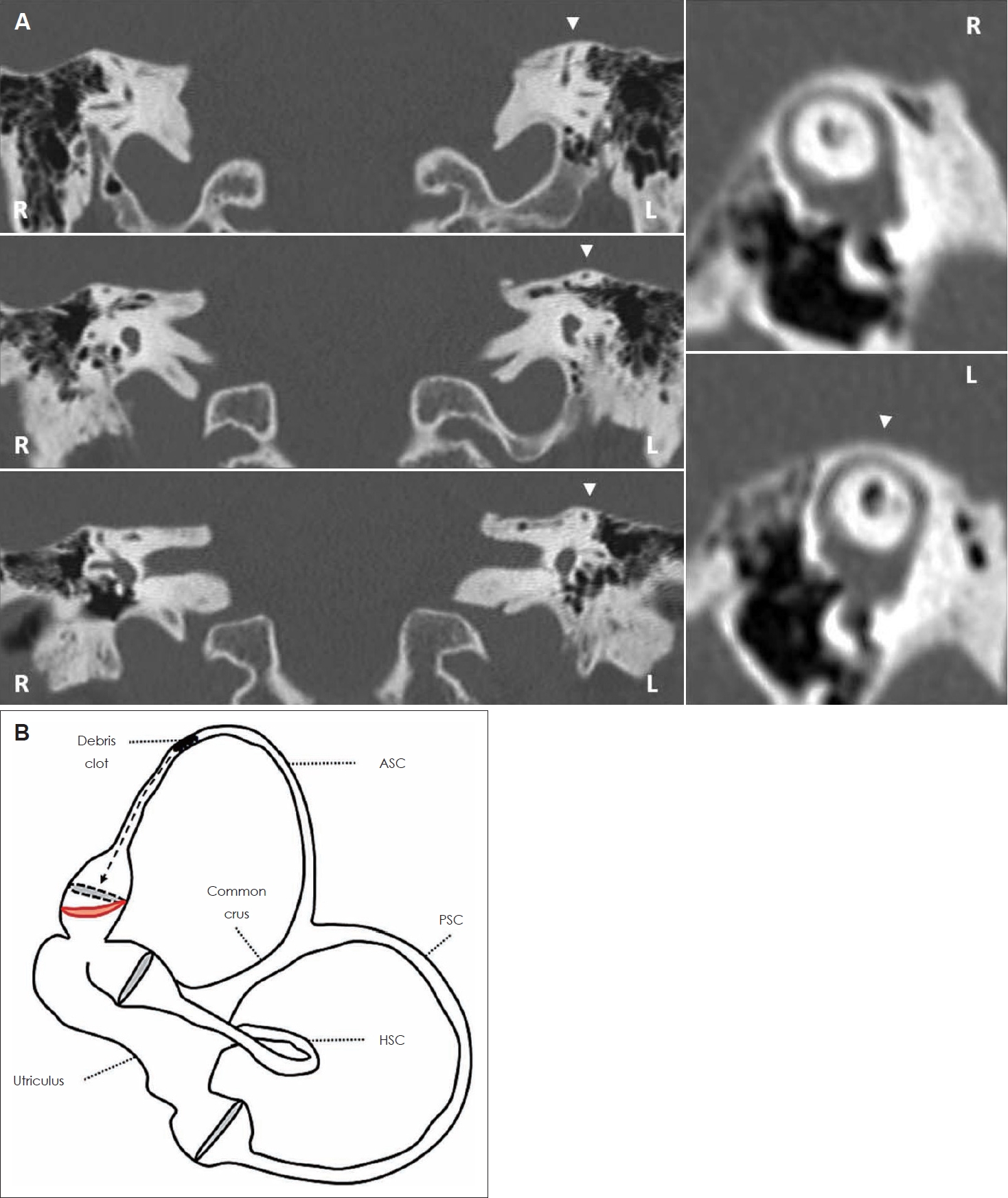
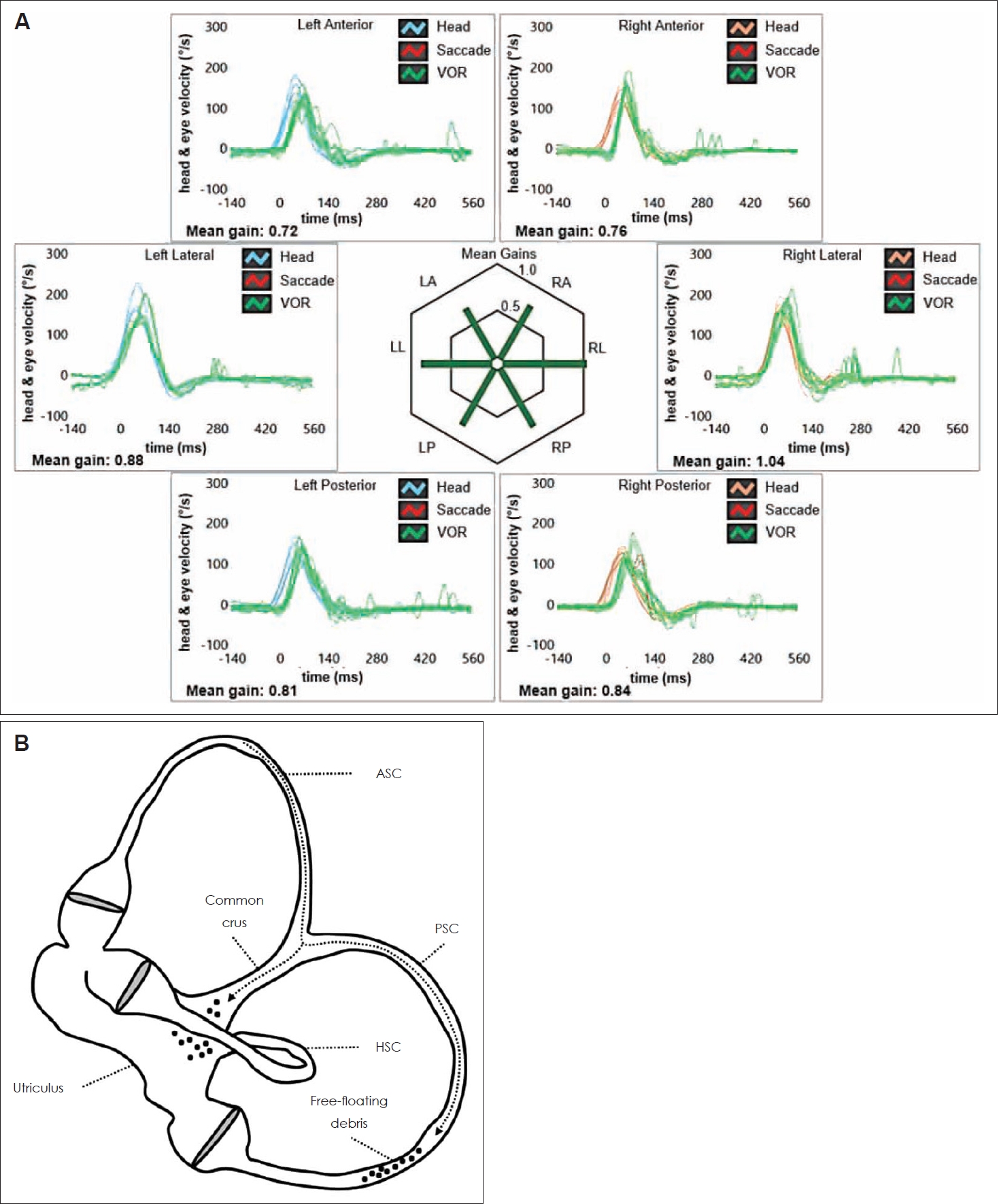
A 56-year-old woman presented at our attention with persistent unsteadiness following canalith repositioning maneuvers (CRM) for relapsing left-sided PSC-BPPV. Her clinical history was uneventful besides arterial hypertension and subclinical hypothyroidism. She denied recurrent headache and significant auditory symptoms. Video-Frenzel examination highlighted spontaneous UBN with subtle right-torsional components not affected by head position changes (Supplementary Video 1 in the online-only Data Supplement). Nystagmus was suppressed by visual fixation whereas it slightly increased its amplitude by skull vibrations and both Dix Hallpike positionings. Bedside testing excluded oculomotor abnormalities and neurological examination ruled out central disorders. Video-HIT performed using the ICS Impulse device (Otometrics, Natus Medical Inc, Taastrup, Denmark) (Fig. 1A) only detected a hypoactive left-sided ASC, whereas cervical and ocular-VEMPs for air-conducted sounds recorded using a 2-channel evoked potential acquisition system (Viking, Nicolet EDX, CareFusion, Heidelberg, Germany) were within normality ranges (Fig. 1B). Temporal bones high-resolution computed tomography excluded bony labyrinth defects (Fig. 2A), whereas brain-magnetic resonance imaging ruled out brainstem/cerebellar abnormalities. A canalith jam (CJ) involving the left ASC was postulated (Fig. 2B). The patient first received weekly sessions of uneventful CRM for ASC-BPPV. Then, she was instructed to perform Brandt-Daroff exercises at home. Some weeks later, unsteadiness receded whereas positional vertigo recurred. Whereas spontaneous UBN disappeared and left ASC hypofunction normalized (Fig. 3A), long-latency and low-amplitude positional UBN with subtle left-torsional components was detected on left Dix Hallpike position (Supplementary Video 2 in the online-only Data Supplement) consistent with left PSC-BPPV (Fig. 3B). She finally received successful Epley’s CRM with symptoms receding.
The authors certify that they comply with the Principles of Ethical Publishing and declare that they acted in accordance with ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Written informed consent was obtained from the patient for the publication of this case report, including all data and images. The local ethical committee of the Azienda USL-IRCCS di Reggio Emilia does not perform formal ethical assessment for case reports.
Discussion
CJ is a rare subtype of BPPV occurring when otoconia are assumed to aggregate, either spontaneously or following CRM, and occlude a narrow canal tract. It results in a persistent deflection (either utriculofugal or utriculopetal) of the cupula and in a blockage of endolymphatic flows between the clot and the cupula itself, generating spontaneous nystagmus [5-7]. While CJ involving the horizontal canal has demonstrated to result in spontaneous nystagmus mimicking an acute vestibular loss [6-8], it has already been reported how PSC-CJ could generate spontaneous DBN overlapping central oculomotor disorders [9-11]. In both cases, a reversible isolated hypofunction for the affected canal on video-HIT has demonstrated to represent a key data in the differential diagnosis [6,9-11]. In fact, according to the pathomechanism assumed for CJ, as the cupula of the affected canal is supposed to be persistently bent either in excitatory or inhibitory direction, dynamic responses of the ampullary receptor would be markedly impaired, leading to a canal “pseudo-hyporeflexia” [5-7,9-11]. Once the otolith clot crumbles, otoconia are free to float again within the canal, without affecting cupular dynamics for the high-frequency domain, thus resulting in a restoration of video-HIT measurements [6,9-11].
To the best of our knowledge, a CJ involving the ASC has never been reported in the literature. In the present case, an ASC-CJ could likely be hypothesized as the underlying pathomechanism. In fact, besides the recent left-sided BPPV suggesting an ipsilesional otoconial dislodgment, a continuous ampullopetal inhibitory flow induced by a persistent positive pressure exerted by the otolith clot over the cupula of the left ASC could likely result in spontaneous UBN with subtle right-torsional components (Fig. 2B). It is reasonable to assume that the debris clot accidentally remained entrapped within a stenotic tract of the ampullary arm of the left ASC to induce a continuous inhibitory ampullopetal flow of endolymph facilitated by the gravity vector. On the contrary, it might be hypothesized that a continuous ampullofugal excitatory flow resulting in a spontaneous nystagmus aligning with the same ASC plane but with opposite direction (downbeating with left-torsional components) could have been expected if CJ had settled a stenotic tract of the non-ampullary arm of the left ASC. In fact, both mechanism (inhibitory and excitatory) have already been described in CJ [5-7,9-11]. The lack of clear right-torsional components in presenting UBN (Supplementary Video 1 in the online-only Data Supplement) is in accordance with ASC-BPPV physiology, as it has been observed how the activation of ASC afferents mainly results in vertical eye movements, probably due to the peculiar geometrical orientation of the ASC and to an upwards bias in vertical slow phase eye velocity [4]. The unresponsiveness to standard CRM supports the assumption of an acquired/structural ASC stenosis preventing a complete release from otoconia. The final conversion in ipsilateral PSC-BPPV with Brandt-Daroff exercises suggests that an impulsive physical therapy was needed to disrupt the clot, allowing debris to overcome the canal stenosis and settle the PSC through the common crus (Fig. 3B). The same pathomechanism could also explain the underlying left ASC hypofunction, normalizing after physical treatment. On the other hand, neuroanatomical networks underlying vestibulo-olcular reflex (VOR) responses coming from the PSC may likely explain the lack of significant left-torsional components in transient positional UBN elicited in left-sided Dix Hallpike position due to the final left PSC-BPPV (Supplementary Video 2 in the online-only Data Supplement). In fact, according to anatomical and physiological data, PSC excitation results in activation of ipsilateral superior oblique and contralateral inferior rectus muscles, resulting in a disconjugate nystagmus with stronger torsional/horizontal components in ipsilateral eye movements and more vertical activity in the contralesional eye [1]. Since we adopted a head-mounted camera with right-eye monocular recording as video-Frenzel, positional nystagmus due to left PSC-BPPV resulted in stronger UBN than left-torsional components. Additionally, long-latency and low-amplitude eye movements evoked in left Dix Hallpike position could likely be explained hypothesizing that a portion of debris eventually fell within the utriculus after Brandt-Daroff exercises, whereas a residual smaller amount of particles crossed the common crus and settled the ampullary arm of the left PSC (Fig. 3B). In fact, according to a mathematical tridimensional model of the labyrinth, the latency of positional nystagmus in case of canalolithiasis would be inversely related to the size of floating particles, while the magnitude of eye movements would be directly related to the number of displaced otoconia [12]. Applying these notions in clinical practice, we could assume that few and small dislodged otoconia are expected to result in positional nystagmus with longer latency and small intensity, as in the case herein reported.
Finally, although ASC-BPPV has been related to positional vertigo rather than persistent unsteadiness as in the present case, it could be assumed that the presenting findings herein described could be attributed to left ASC-cupulolithiasis, where otoconia are thought to adhere to the cupula overloading it. Nevertheless, both ASC-canalolithiasis and cupulolithiasis should only result in positional DBN (either lasting less than 1 minute or persisting for more than 1 minute, respectively) after both Dix Hallpike and straight head hanging positionings, sometimes reversing when returning upright [1,4]. On the contrary, our patient presented with spontaneous UBN with slight right-torsional components enhanced by positioning tests, not reversing with head position changes. These findings could be explained neither by ASC-cupulolithiasis nor by ASC-canalolithiasis. The only possible mechanisms involving dislodged otoconia include either a continuous inhibitory endolymphatic flow bending the cupula of the left ASC towards the utricle due to left ASC-CJ or a continuous excitatory utriculofugal deflection of the right PSC cupula due to right PSC-CJ. Since the patient was previously treated for refractory left-sided PSC-BPPV and due to left ASC VOR-gain reduction consistent with CJ pathomechanism, it is reasonable to assume the first picture as the most likely hypothesis.
Although a selective ASC hypofunction on video-HIT has already been described in other peripheral pathologies including endolymphatic hydrops [13] and superior canal dehiscence [14], both conditions were excluded by clinical-instrumental data and imaging, respectively. Moreover, as central vestibular disorders have hardly demonstrated to result in a selective ASC hypoactivity [15], no other labyrinthine pathologies could likely result in spontaneous UBN with such a reversible lesion pattern.
In this report, we described how the use of a comprehensive vestibular assessment enabled to recognize a unique labyrinthine disorder as the underlying pathomechanism. Besides distinguishing from central disorders, a selective ASC hypofunction on video-HIT allowed to hypothesize an ASC-CJ and to treat the patient accordingly, providing further insights to the pathophysiology of spontaneous UBN of peripheral origin. Unfortunately, vestibular examination was conducted only with Video-Frenzel goggles, without a video-nystamographic acquisition system. Therefore, we could not provide nystagmographic data for spontaneous nystagmus (such as slow phase velocity) and for modulation of nystagmus amplitude according to positional changes and skull vibrations. Even though further investigations are needed before any conclusion can be reached on the clinical value of video-HIT in case of spontaneous nystagmus along the vertical plane, we can suggest to consider CJ involving the ASC in the differential diagnosis of spontaneous UBN, in particular if it is associated with previous BPPV and isolated ASC hypofunction on video-HIT.