Introduction
Childhood hearing loss can seriously affect language development. Early detection of a hearing problem with a diagnostic tool like newborn hearing screening test is important. Early detection can bring improvements in hearing ability and language development of children by promoting the use of rehabilitation strategies including hearing aid and cochlear implant.
Auditory neuropathy is characterized by abnormal auditory brainstem response (ABR) and normal otoaoustic emission (OAE) responses. Although auditory neuropathy manifests as various patterns in pure tone and speech audiometry, most patients have very poor word discrimination function.1)
We present a case of auditory neuropathy improved in a child who was diagnosed with moderate hearing loss by ABR testing at 16 months of age, but who presented normal pure tone threshold and speech discrimination score 3 years after wearing hearing aids.
Case Report
A six-year-old boy presented to the outpatient clinic with abnormalities of hearing and language development. The patient was born vaginally at 40 weeks. No congenital anomalies were evident at birth. However, he was not able to speak until 16 months of age and his response to external sound stimuli was slow. He showed no ABR-response to 65 dB nHL click stimuli at 16 months age. Since then he had worn a hearing aid in the right ear (Fig. 1). At 25 months of age, aided hearing threshold was about 30 dB HL in sound field pure tone audiometry (Fig. 2). He wore the hearing aid for another 2 years.
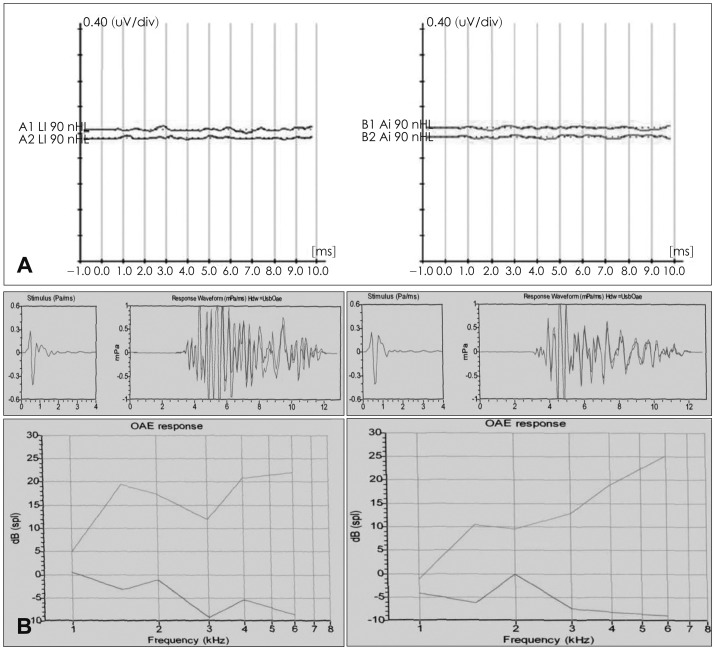
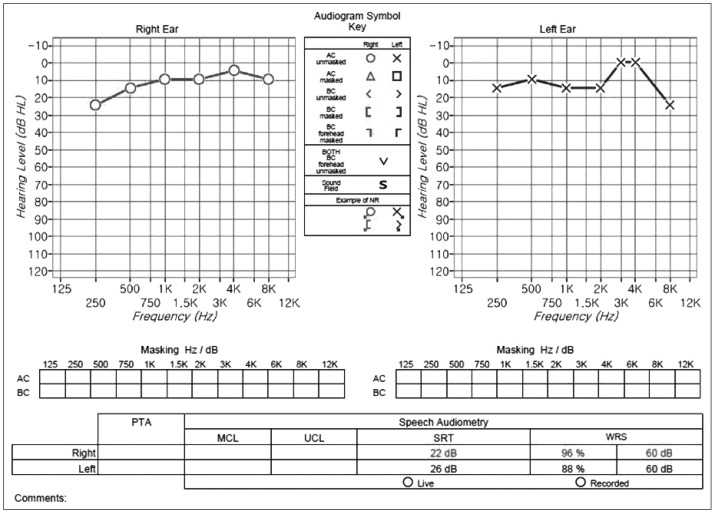
At 5 years, 10 months of age, he visited our hospital for a hearing evaluation. His parents related that his hearing function seemed to have improved with time, because he had no difficulty communicating with others without a hearing aid. Physical examination revealed that both tympanic membranes were normal. ABR test showed no click sound response in both ears at 90 dB nHL (Fig. 3A). Transient evoked otoacoustic emission showed response reproducibility of 88% (right ear) and 95% (left ear), and normal distortion product otoacoustic emissions responses were reported (Fig. 3B). These results were compatible with auditory neuropathy. However, normal pure tone threshold was evident at both ears; speech reception threshold was 22 dB (right ear) and 26 dB (left ear) and speech discrimination score was 96% (right ear) and 88% (left ear) (Fig. 4). He was recommended to stop wearing the hearing aid. A language development test conducted at 7 years, 4 months of age revealed an age equivalent of 6 years on expressive vocabulary test and 5 years on receptive vocabulary test. Language developmental delay and mild phonological disorder were diagnosed. He is still participating in language therapy
Discussion
The concept of auditory neuropathy was first introduced by Starr, et al.1) in 1996 to describe 10 patients, including infants and adolescents, showing normal OAE results, abnormal ABR results and poor speech discrimination score. Auditory neuropathy is characterized by the auditory pathway lesion in the inner hair cells, the junction between the inner hair cells and the nerve, and the spiral ganglion or the auditory nerve in the presence of normal outer hair cell function. Lesions can be single or multiple. From a pathophysiological point of view, auditory neuropathy is described as peripheral neuropathy resulting from the demyelination of auditory nerves. Demyelinating lesions decrease the speed of neurotransmission, which in turn impairs nerve stimulation responses of the brain stem and decreases the synchronized activity of the entire auditory nerve activity, leading to unusual waveforms.1,2)
Auditory neuropathy accounts for nearly 2.4-15% of all childhood sensorineural hearing loss. Auditory neuropathy most often occurs in both ears among infants aged 2 years or younger although it can occur in adults.3) More recently, auditory neuropathy has been increasingly referred to as auditory neuropathy spectrum disorder in recognition of its heterogeneity. Auditory neuropathy is multifactorial includes generic, congenital and acquired risk factors. These risk factors include hypoxia, preterm birth, hyperbillirubinemia, ototoxic medication use and neurological diseases, such as mitochondrial disease. Especially, hyperbilirubinemia is a leading cause of auditory neuropathy.4) Infants with one of these risks need to undergo OAE testing, especially when they have a poor ABR Roche, et al.5) reported the relationship of radiologic findings with auditory neuropathy in 118 patients; radiologic abnormalities were observed in 64% and 23% of patients examined using magnetic resonance imaging (MRI) group and computed tomography, respectively. The most common abnormality in MRI is the absence of the auditory nerve, followed by brain lesion. MRI is the most important radiologic tool in deciding on a course of treatment and assessing the prognosis of auditory neuropathy. In this case, radiological examination was not conducted for the patient.
The treatment for childhood auditory neuropathy includes hearing aids, language therapy and regular hearing test-based monitoring. Also, cochlear implant can be considered in case of poor outcomes.6) Kim, et al.7) compared outcomes of six children with auditory neuropathy and four children with sensorineural hearing loss after cochlear implant, and reported no difference in hearing recovery outcomes between the two groups. Fulmer, et al.8) also reported no significant difference in hearing improvement following cochlear implant in 10 patients with auditory neuropathy and 10 patients with sensorineural hearing loss.
For infants, ABR waveforms can be improved with time, so hearing conditions should be tested and examined regularly. Dunkley, et al.9) introduced a case in which a child showed pure tone threshold average of 35 dB HL and normal word discrimination test 5 years after the diagnosis of audiometry neuropathy based on ABR waveforms of 50 dB nHL with normal OAE at 1 week of age. Psarommatis, et al.10) also chronicled the improvement of auditory neuropathy in 20 children of 25 patients who had ABR waveforms of more than 75 dB nHL and normal OAE. Of the 20 children, 12 exhibited ABR less than 40 dB nHL and one child had 50 dB nHL but normal results in other hearing tests. Berlin, et al.11) studied 260 children with auditory neuropathy and found that 13 (5%) had no problem in language development and ended up needing no treatment, even hearing aids. The patient in the present case also showed typical clinical features of auditory neuropathy including non-response for ABR in addition to normal OAE results. However, hearing improved to the extent that he had normal hearing for puretone and speech audiometry, and language development was only mildly delayed compared to other children in the same age group. We suggest following observation on a regular basis and reassessment of audiologic status and language development.