Introduction
Granulomatosis with polyangiitisis (GPA) is an idiopathic systemic form of vasculitis characterized by involvement of the upper and lower airways and the kidneys. The exact cause of GPA is unknown, but it seems to have characteristics of an autoimmune disease [1].
ENT manifestations are present in the vast majority of patients (73-99%), and are usually among the first symptoms [2]. Occasionally, ear conditions are the first and only manifestations [3]. Therefore, ENT physicians have a determining role in recognizing the early onset of this disease and starting the proper therapy.
Current first line induction therapy for GPA consists of cyclophosphamide with glucocorticoids, which is successful in most (70-90%) patients [4]. However, patients resistant to this regimen may be difficult to treat. Although a few patients presenting with otologic symptoms and treated with conventional therapy, such as cytotoxic drugs and steroids, have been described, this case was a rare and meaningful report in otology to date of a patient presenting with unilateral facial nerve palsy and bilateral profound sudden sensorineural hearing loss with vertigo.
We describe here a patient with a resistant fulminant generalized form of GPA initially presenting as bilateral sudden sensorineural hearing loss and facial palsy. Treatment of this patient with rituximab resulted in significant clinical improvement.
Case Report
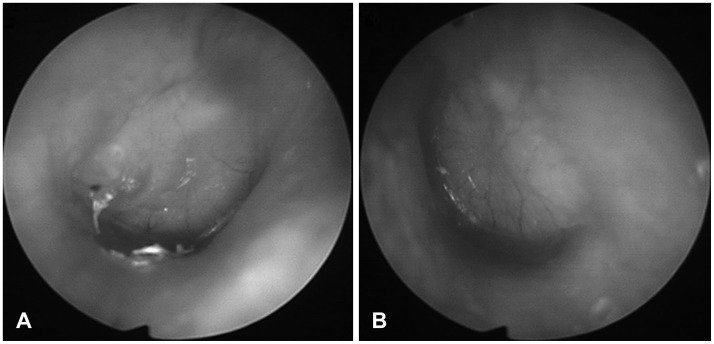
A 47-year-old man visited our hospital due to symptoms of facial paralysis on the left side and abrupt hearing disturbance with dizziness in both ears three days earlier. In physical examination, both tympanic membrane were bulging (Fig. 1). At the time of visit to our hospital, impedance audiometry (Grason-Stadler GSI 33 middle-ear analyzer; Viasys, Conshohocken, PA, USA) was B-type on both sides; and pure tone audiometry (Grason-Stadler GSI 61 clinical; Nicolet Biomedical, Madison, WI, USA) was 95 dB on the right side and off scale on the left side (Fig. 2A). Tests of auditory brainstem response found that the right side formed a V-wave at 80 nHL, whereas the left side did not form a V-wave at 90 nHL. Computed tomography scans (General Electric Medical Systems, Milwaukee, WI, USA) showed dense fluid in both external ears and middle ears but no facial canal dehiscence (Fig. 3).
The patient was started on 80mg/day oral steroids for 12 days. Simple chest X-rays showed multiple nodules in both lung fields, while CT of the chest showed that chest cavity was filled with multiple nodules (Fig. 4A, B). Immunological tests showed significantly higher than normal proteinase-3 anti-neutrophil cytoplosmic antibodies (ANCA) representing c-ANCA. A definitive diagnosis required a lung biopsy sample. However the patient refused further evaluation.
Following discharge from the hospital, the patient began coughing severely and developed a continuous fever of about 38℃. In addition, hearing ability again deteriorated. Chest CT showed increased size and number of nodules in the fine structure of the lungs (Fig. 4C, D). A lung biopsy sample was obtained, and he was started on high-dose intravenous steroids 500 mg/day for three days. After six days, C-reactive protein (CRP) tended to decrease from 18.04 to 4.36, but he showed no improvement in other symptoms including fever.
A lung biopsy taken on day six showed necrotizing granulomatous inflammation with intra alveolar hemorrhagic exudates and capillaritis (Fig. 5), resulting in a diagnosis of GPA. The patient was started on 1000 mg/day cyclophosphamide, along with steroids, two-week interval. However, erythrocyte sedimentation rate, CRP and fever all remained high. He was therefore administered four infusions of rituximab (Mabthera; Roche Pharma, Basel, Switzerland, 500 mg each), an anti-CD20 monoclonal antibody, at two week intervals, along with concurrent IV cyclophosphamide (Endoxan; Bukwang Pharm, Seoul, Korea, 500 mg twice a month for 3 months). After rituximab administration, symptoms including cough, fever, and otologic symptoms, improved significantly. To improve hearing, he received seven intratympanic injections of steroids through the ventilation tubes in each ear. After four months, pure tone audiometry improved on the right side to 32 dB (Fig. 2B) but did not improve on the left side, and left side facial paralysis improved from HB grade 5 to HB grade 2. Written informed consent was obtained from the patient who participated in this case.
Discussion
GPA is a relatively rare disease, so treatment focusing on local symptoms in the absence of an accurate diagnosis may have no effect, or even worsen the disease, with the possibility of a secondary infection. Thus, an accurate initial diagnosis and subsequent treatment with steroids and, if necessary, immunosuppressive drugs, are important.
The American College of Rheumatology (ACR) criteria for confirming the diagnosis of GPA was found to have a sensitivity of 88.2% and a specificity of 92%. A diagnosis of GPA requires at least two of the following four criteria: 1) hematuria (more than 5 red blood cells per visual field or the presence of erythrocyte casts), 2) changes in chest radiographs, 3) ulceration of the mouth and/or nose, and 4) positive histopathological examination. In addition about 80-90% of these patients are positive for ANCA, which damage vascular endothelium and cause its necrosis [5].
In evaluating our patient, we initially focused on the areas usually involved in GPA, including the upper and lower airways and the kidneys. A lung biopsy sample taken from our patient showed necrotizing granulomatous inflammation with intraalveolar hemorrhagic exudates and capillaritis. He also had intranasal inflammation and nodules and cavities in the chest, thereby satisfying more than two of the four ACR criteria.
Ear disorders may be the first and only manifestation of GPA. Otologic involvement may include otitis media with effusion, chronic otitis media, sensorineural hearing loss, vertigo, and/or facial palsy [3]. Proposed mechanisms include cochlear nerve compression by an adjacent granuloma, cochlear immune-complex deposition, and local vasculitis involving cochlear vessels. Progression is generally rapid; however, the condition is occasionally reversible with glucocorticoids or cytotoxic agents [3]. Our patient presented with the otologic symptoms of unilateral facial palsy and bilateral sudden sensorineural hearing loss with vertigo.
Hearing loss was likely due to recurrent serous and/or suppurative otitis media and/or sensorineural hearing loss. Sensorineural and conductive hearing loss occurred with similar frequencies, 47% and 33%, respectively, but the latter showed a better response to treatment, indicating a poorer prognosis in patients with sensorineural hearing loss [6]. The right side hearing threshold in our patient improved to 32 dB, but left side showed no improvement.
Facial nerve palsy in association with GPA is rare, being present in about 5% of patients, either alone or in combination with hearing loss; rarely, facial nerve palsy may be the presenting feature. Facial nerve palsy is secondary to compression of the nerve in the middle ear, especially in the presence of a dehiscent facial nerve canal or due to vasculitis [7]. Differential diagnosis is important in patients with facial nerve palsy; other diseases should be considered, such as chronic otitis media and systemic vascular diseases, including sarcoidosis, polyarteritis nodosa and tuberculosis [8].
The standard treatment for systemic GPA is an immunosuppressive drug such as cyclophosphamide to alleviate the disease, along with a glucocorticoid. If these regimens are ineffective, the patient should be treated with rituximab [9], a chimeric monoclonal antibody directed against CD20 that induces B cell apoptosis and depletion in peripheral blood. The importance of ANCA in the pathogenesis of GPA suggests that rituximab reduces ANCA by depleting B cell concentrations. Our patient was initially treated with cyclophosphamide and a glucocorticoid, but symptoms worsened. Addition of rituximab improved symptoms dramatically.
GPA is a rare but dangerous disease, which may progress rapidly if misdiagnosed. This study describes a patient with a rare type of multi-organ involved, treatment resistant, fulminant form of GPA initially presenting as bilateral profound sudden sensorineural hearing loss with vertigo and unilateral facial palsy and illustrates the dramatic effects of rituximab.