Introduction
Bone conduction hearing aids can transmit sound vibrations directly to the inner ear through the skull, thereby bypassing any conductive impairment in the external or middle ear [1]. Patients with recurrent otitis media or otitis exacerbation find it difficult to wear conventional air-conduction hearing aids. Moreover, compared to bone conduction implants (BCIs), conventional hearing aids have disadvantages such as the damping of sound vibrations by the hearing aid and the inconvenience due to irritation of the attachment area. BCIs are good alternative options for these patients [2,3]. Since the successful placement of the first implant was reported in 1977, more than 10,000 patients worldwide have received BCIs [1]. In addition, conventional bone conduction hearing aids, such as the soft Headband, are a gold standard for preoperative evaluation in young patients who cannot undergo implantation and are used as a good method for hearing rehabilitation in patients refusing surgery [4,5].
To maximize the gain of sound conduction, the bone conduction vibrator should be kept under a constant pressure (approximately 2-5 N) on the head [6]. The shape of the headset body determines the degree of contact and pressure between the head and the device, and it plays an important role in the efficacy of sound transmission. Although many bone conduction hearing aids have been developed and used, most of them are foreign products designed for different populations; hence, they are not suitable for the heads of Korean adults. Studies have also shown that, compared to the Caucasians, Asians have heads that are more round, with flatter foreheads and backs [7]. Therefore, products designed using different population data may not be suitable for Koreans.
The human body measurement research project for Koreans is currently in progress and in its 7th stage. This project has yielded useful data for designing products and devices in various medical fields. However, among the Korean human body measurements, the head size measurements may present some limitations. The head size was mainly measured in people aged less than 69 years old, with relatively less data being collected from the elderly. Moreover, the project determined the size of the head by using five criteria, which did not account for the actual wearing position of the bone conduction headset. Furthermore, the thickness of the temporal bone to which the BCI was applied to could not been determined.
Human anthropometric measurements determined using computed tomography (CT) images have been reported in various studies [8]. In particular, CT enables the measurement of any diameter of the skull bones that cannot be measured directly. In this study, we measured the head dimensions on CT images and compared them to direct measurements of the human head. We aimed to supplement existing head size data with data from our analyzed parameters on CT images and to predict a new parameter of bone thickness for aiding BCI placement.
Subjects and Methods
Patients
This study was performed at Wonju Severance Christian Hospital and was approved by the Institutional Review Board (CR318037). Facial and mandibular bone CT images of patients acquired between January 1, 2017 and July 1, 2018 were reviewed. The patientsŌĆÖ age at the time of acquiring the CT images had to range from 10 to 90 years old, because we aimed to classify the head sizes according to the ages ranging from the 10s to the 80s.
The exclusion criteria were as follows: 1) images that did not include a vertex and could not be used to measure the skull size; 2) patients with a past history of conditions affecting skull size measurement, e.g., skull fracture or brain surgery; and 3) patients without clinical data such as weight and height. Finally, we enrolled 406 patients in this study. The age of the patients ranged from 10 to 88 years, and their mean age was 48.58┬▒22.24 years. Of the 406 patients, 221 (54.4%) were males and 185 (45.6%) were females. Patients were divided into groups according to age and included 42 to 63 people in each group (10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, and 80-89).
The 6th Size Korea project included measurements from 14,016 people (7,532 males and 6,484 females) aged 7 to 69 years old, whose head size parameters were directly measured. Using propensity score matching, considering the height and weight of the experimental group, we were able to select 1,218 matched individuals, i.e., three times the number of patients with CT data.
Measurements in the Size Korea project
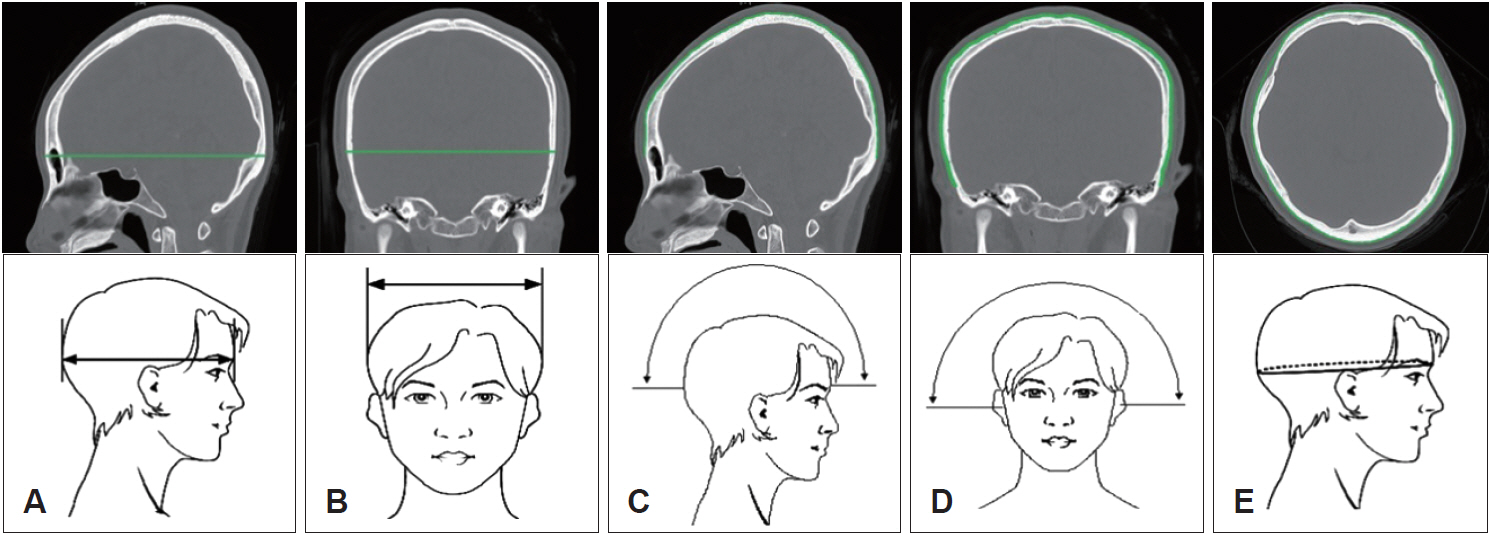
The 6th Size Korea project included five parameters related to skull size, namely, head length, head width, sagittal arc, bitragion arc, and head circumference. The definitions of the measurement parameters and the measurement reference points are summarized in Table 1.
1) Head length: The distance from the glabella to the occiput
2) Head width: The horizontal distance between the right and left euryon
3) Sagittal arc: The length from the glabella to the inion
4) Bitragion arc: The length from the right tragion, passing the vertex, to the left tragion
5) Head circumference: The perimeter through the glabella and the occiput
Two experimenters were trained to become accustomed with the measurement tools and procedures. The features were initially identified as skeletal landmarks on the face. Measurements were obtained to the nearest millimeter and were recorded in centimeters. Normally, the investigators worked in a private room to provide the subject the most preferable environment. All subjects were provided a non-disclosure agreement to preserve their names.
Measurements on the CT images
Facial and mandibular bone CT was performed using GE Light Speed Pro 16 (GE, Milwaukee, WI, USA) and Philips Brilliance 64 (Philips, Cleveland, OH, USA) (thickness, 2.5 mm). The patients underwent axial topography parallel orbito-meatal line scanning in the normal supine position. Coronal and sagittal images were reconstructed perpendicular to the orbital plane and perpendicular to the axial plane, respectively.
The five skull-size-related parameters were measured on facial and mandibular bone CT images. We additionally measured temporal bone thickness, which could not be directly measured. Temporal bone thickness was measured at a point 3 cm posterior and 2 cm superior to the posterior wall of the external auditory canal (EAC), which is the typical location of BCI placement.
These measurements were performed by two separate researchers. The lengths of straight-line parameters (head length, head width, and thickness) were measured using the Centricity software (Centricity; GE Medical Systems, Milwaukee, WI, USA), and the lengths of curved parameters, such as head circumference, bitragion arc, and sagittal arc, were measured using Image J (National Institutes of Health, Bethesda, MD, USA). The measurements were based on the bone rather than the soft tissue.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA). Propensity score matching was performed, and a 1:3 ratio matching (CT group:Size Korea group) was done considering the height, weight, and body mass index of the CT group. A paired t-test was performed to analyze the two groups. A p-value less than 0.05 was considered to indicate a significant difference.
Results
Comparison of measurements of head size between the Size Korea project and the CT images
The measured head size parameter values are provided in detail in Table 2. The head size parameter values measured on CT images were significantly smaller than those measured directly on the human body. The average difference was the greatest for head circumference at 49.5 mm (552.45┬▒13.17 mm in the Size Korea measurement and 502.80┬▒24.26 mm in the CT measurement; p<0.001), and it was the smallest for head length at 7.85 mm (178.42┬▒6.21 mm in the Size Korea measurement and 170.86┬▒8.30 mm in the CT measurement; p<0.001).
Changes in head size parameters in the CT images according to age
The differences in four parameters (except for head length) between the two groups according to the age groups were not statistically significantly different. The changes in head size parameters measured on CT images according to the age groups are presented in Table 3. The relationship between the Size Korea projectŌĆÖs directly measured data and CT data according to the age groups is shown in Fig. 2. This implied that all measurements, excluding the soft tissues, performed in the Size Korea project were consistent with the measurements we performed on CT images. The head lengths measured on CT images in young patients (ages in the 10s and the 20s) were considerably larger than those in the Size Korea data. This could be because in the Size Korea data, the measurements of human body size showed a steep increase until the 20s, showing the highest values, but gradually decreased thereafter from the 30s.
Prediction of temporal bone thickness in Koreans according to age groups
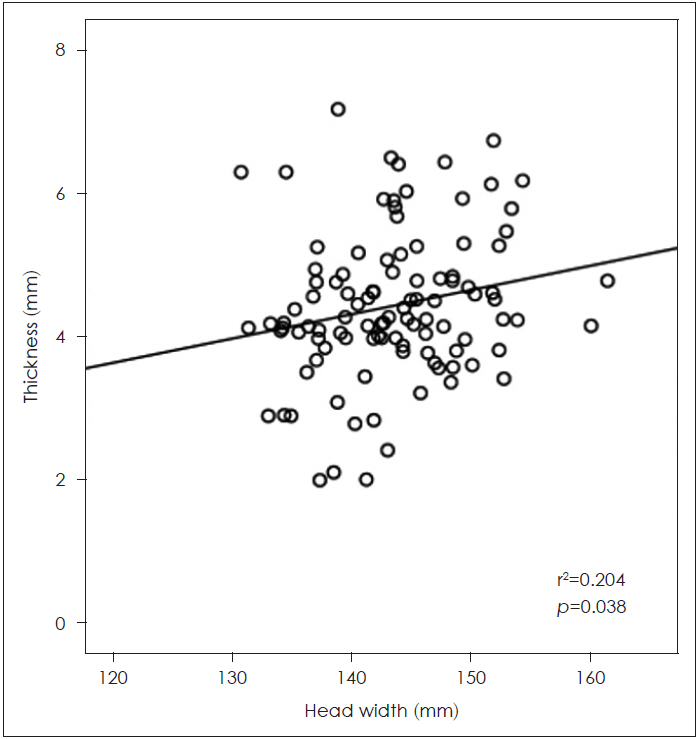
We measured temporal bone thickness for aiding BCI placement by using CT data, because it cannot be directly measured using the Size Korea data. Bone thickness is an important factor that determines the benefit of sound gain as well as the surgical indication for BCI placement. The highest value was 4.89┬▒0.93 mm in the 70s and the lowest value was 4.10┬▒0.99 mm in the 10s (Table 3). Correlation analysis (Fig. 3) was performed between the five head size parameters and temporal bone thickness, and only head width showed a significant correlation (r2=0.204, p=0.038).
Discussion
Bone conduction hearing aids transmit sound vibrations through the skin to the skull bone, and further to the cochlea in the inner ear, bypassing any conductive impairment in the external or middle ear [9,10]. Therefore, bone conduction hearing aids or headsets are an option for treating deafness. Recently, non-invasive bone conduction hearing aids, such as the Baha SoundArc (Cochlear, Sydney, Australia) and Adhear (MED-EL, Innsbruck, Austria), have been designed to be placed over the ears and be worn behind the head [2,11]. SoundArc demonstrated equal performance to the Softband and superior performance to the Headband and Testband [12]. The performance of nonsurgical bone conduction solutions relies mainly on two factors: sound transfer efficiency and minimizing feedback. To solve these problems, bone conduction devices should be attached to the mastoid area with appropriate pressure to transmit the sound, and the contact force should be about 2-5 N [6]. Bone conduction devices should be fixed without any gaps at the attachment site; otherwise, they will have a negative impact on sound transmission. Head size is an important point to consider when developing devices such as bone conduction headsets and hearing aids. Most bone conduction devices are designed using reference standards obtained from foreign patient populations. Therefore, such devices may not have the maximum efficiency when used in Korean patients with different head sizes. Therefore, to develop a product suitable for Koreans, the establishment of a reference standard for the Korean head size is pertinent. Although the Size Korea project provides head size data, these are not widely used because they have limited applicability when developing medical devices. Temporal bone thickness data should be obtained to plan the position of BCIs and accomplish a successful surgery.
Anthropometric data are important factors in the design of medical devices. However, in reality, head and face shapes differ between individuals of different nationalities. Therefore, it is imperative to consider these differences in areas of object, system, and environmental design. Few studies have calculated the Korean head size. A single photon emission CT study on children suggested a series of Korean computational head phantoms with detailed cranial substructures [13]. Lee, et al. [5] showed that the face and head sizes of Korean male and female individuals have more statistically significant morphological differences than do those of Japanese individuals. Since 2003, the Korean anthropometric data survey project named Size Korea has provided Korean body size reference data, including head size data. Knowledge of the human head form is essential in a variety of fields like design and medicine [7,14]. However, the Size Korea project included only five head size parameters, which limited their applicability when designing medical devices, especially BCIs.
We thought that the measurement of head size on CT images could provide additional reference data to complement the Size Korea projectŌĆÖs anthropometric data, and hence, we compared the head size data measured on CT images to those directly measured for the Size Korea project. In this study, the values measured on CT images were lower than the corresponding Size Korea values. We think that the CT values were lower because 1) we measured the size of the bone rather than the soft tissue and 2) the measurement points were not exactly identical between the two measurement groups; moreover, errors may have occurred during the measurements. Although the measured CT values were smaller, the five head size parameters in both the groups showed a similar tendency when viewed on the numerical graph based on the age groups. The observation of a similar tendency according to the age groups shows the reliability of the CT measurement method.
We think that CT measurements have some strengths over direct measurements. CT enables the measurement of bone sizes that are impossible to measure directly. This would be meaningful when designing bone conduction devices, which should have a contact with appropriate pressure on the bone. In addition, we could obtain and include data from patients in their 70s and 80s, and could determine new parameters such as temporal bone thickness without re-imaging [15]. Therefore, if sufficient CT data are available in the future, they could complement national reference data (such as the Size Korea data) when developing bone conduction devices for the Korean population.
A limitation of this study was that most of the patients with CT data were from the Chungbuk or Gangwon provinces. Therefore, these patients are not representative of the whole Korean population. However, there is no evidence showing that head size changes in different regions of Korea. Therefore, we think these data can serve as meaningful standards for the Korean population.
The position of bone conduction devices is important, because it plays a role in sound transmission. According to the literature, the proximity of a bone conduction device to the cochlea is important in improving the amplification of the signal provided to the cochlea [16]. Simultaneously, avoiding the sigmoid sinus can prevent bleeding and epidural hematoma [17]. In this study, we measured temporal bone thickness at a point 3 cm posterior and 2 cm superior to the posterior wall of the EAC, where BCIs are usually placed [18]. The mean thickness ranged from 4.10┬▒0.99 mm to 4.89┬▒0.93 mm, showing sufficient depth for BCI placement. The correlation between the five parameters and temporal bone thickness showed that bone thickness increased only with an increase in head width (r2=0.204, p=0.038).
In conclusion, the CT-based measurement method described here may help uncover important predictive factors through modeling, and it may be useful for analyzing not only bone thickness but also other important parameters. If more CT data are accumulated in future studies, they could be used in studies to identify numerical associations between head size parameters and to develop predictive factors for specific items (e.g., temporal bone thickness). Moreover, when used together with the Size Korea data, our CT data will aid the development of specific bone conduction headsets for Koreans.