Introduction
Sudden sensorineural hearing loss (SSHL) is a loss of hearing more than 30 dB in at least 3 consecutive frequencies within 3 days. SSHL for which no cause has been found despite appropriate quests is called idiopathic sudden sensorineural hearing loss (ISSHL). Currently, etiology and pathogenesis of ISSHL have not been fully elucidated. For this purpose, many biochemical, clinical, and radiological studies have been conducted [1]. However, it is not yet understood who is more susceptible to ISSHL, unlike who will have the better prognosis. ISSHL was widely accepted as primarily caused by impaired hair cell function however in several studies [2,3], hair cell injury could not be shown in every ISSHL patient. Spiral ganglion neurons and cochlear nerve (CN) neuron dysfunction significantly contributes to ISSHL as described in the following.
Recent studies have demonstrated the clinical significance of morphometric changes detectable by magnetic resonance imaging (MRI) in the CN. The use of MR in patients recently affected with SSHL enabled the detection of morphometric changes in the CN. In principle, the primary goal of MRI in patients with SSHL is to rule out an acoustic neuroma, a necessity before labeling such a hearing loss (HL) as being ISSHL. Besides, an MRI of the CN has usually been performed in profoundly hearing-impaired individuals before cochlear implantation. For instance, reports were obtained in patients with long-standing HL [4,5]. CN imperfection has been demonstrated in congenital as well as acquired sensorineural hearing loss (SHL) patients [6]. Russo, et al. [5] and Kim, et al. [7] highlighted the change in the morphometric measurements of the CN in people with HL for a long time, in adults as well as children. Moreover, Islamoglu, et al. [8] measured CN size in long-lasting single-side deafness due to ISSHL and found no difference between healthy and diseased ears. However, in none of the studies conducted so far, CN size has not been measured and compared with both the healthy side of ISSHL patients and in healthy individuals. In addition, no comparison was made between the pretreatment audiogram type and treatment responses with the CN size.
The current research aimed to evaluate the size of the CN in patients with ISSHL. To this end, CN size was measured in ISSHL patients and compared with the healthy side and the control group, using three-dimensional constructive interference in a steady-state (3D-CISS) sequence on MRI. In addition, the relationship of CN size with pretreatment audiograms and treatment response was investigated.
Subjects and Methods
The present study was conducted in a tertiary referral center after the approval of the local ethics committee (No: 86/05:20.04.2020). Written informed consent was taken from research participants. This research which involves human participants complies with the 1964 Helsinki declaration and its later amendments.
Patient selection
Patients who were diagnosed with ISSHL in 2015â2019 were included in this study. Unilateral 30 dBHL that developed in at least 3 consecutive frequencies in the last 3 days was considered SSHL. Records of the pretreatment and posttreatment audiograms, otologic examination, and contrast-enhanced MR images at the time of the first admission were noted. Patients with bilateral SSHL, vestibular schwannoma, a history of acoustic trauma, otologic surgery, Meniereâs disease, migraine, chronic otitis media, usage of ototoxic drugs, malignancy, and stroke were not included in the research. The control group was composed of age and sex-matched patients who went through temporal MRI studies during the same time frame. Facial palsy, and Meniereâs disease were the exclusion criterias for the control group.
All participitants involved in the study were assessed for vertical diameter (VD), horizontal diameter (HD), and cross-sectional area (CSA) of the CN, as demonstrated by the 3DCISS sequence on MRI. Measurements were evaluated on both sides of all participitants. Also, demographics, ear side with HL, concomitant audiovestibular symptoms such as vertigo and tinnitus, and comorbidities kind of diabetes mellitus and hypertension were analyzed. In the study group, 26 (21%) patients had tinnitus and the other 16 (13%) patients had vertigo with HL as initially. Only 10 (8%) patients had diabetes mellitus, and the other 9 (7%) patients had hypertension in the study group. However, these few numbers of cases were not sufficient for statistical evaluation.
MRI
The imaging examinations was performed on a 1.5-T unit MR scanner (Magnetom Aera, Siemens, Erlangen, Germany), with a 20-channel head coil within 48 hours of admission of patients with ISSHL. Morphometric analyses of the CNs were performed on the 3D-CISS images (repetition time/echo time: 1,200/271, field of veiw: 170 mm, flip angle: 150°, voxel size=0.3Ã0.3Ã0.3 mm).
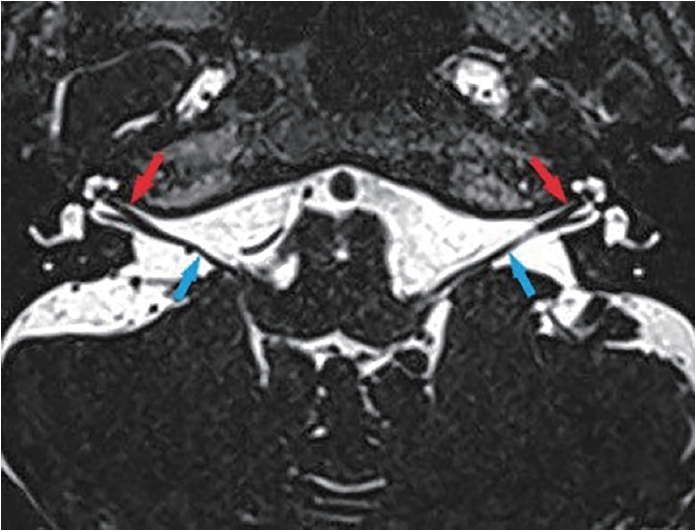
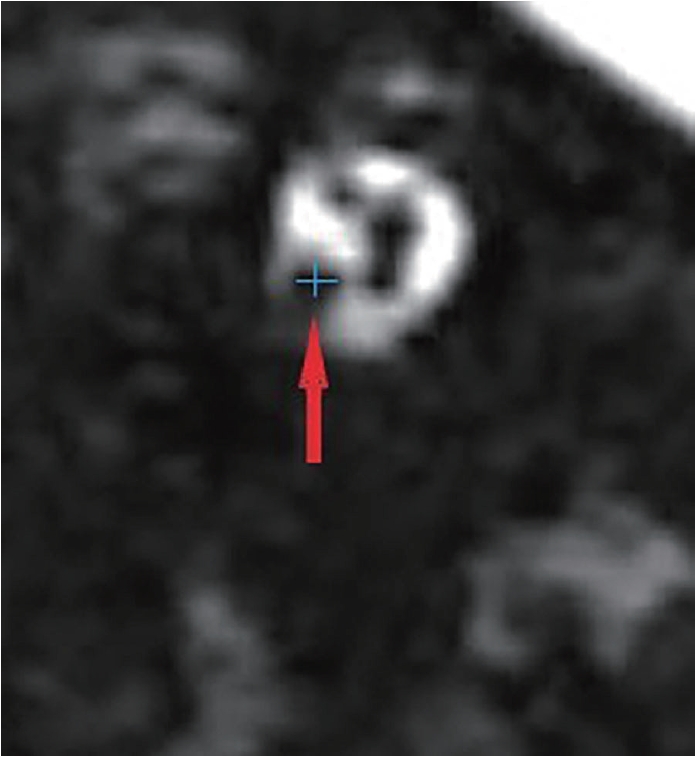
Two national board-certified radiologists (M.Ã. and R.P.K.), who were blind to the group of participants evaluated the images separately and the average of these values was used in the analysis. Measurements were performed twice by Reader 1 with a 1-month interval to assess the intraobserver variability. To examine interobserver variability, measurements performed by Reader 2 were compared with the first set obtained by Reader 1. Measurements were then averaged for both readers. They performed the measurements on the picture archiving and communication system (ExtremePacs, Ankara, TÞrkiye). Initially, to make the measurements, the CN was identified on the axial image shown in Fig. 1. After that, a parasagittal oblique image of the internal acoustic canal (IAC) was formed by using the multiplanar reformation tools. The location of the CN closest to the fundus of the IAC where the CN could separately be identified, was fixed and measurements of VD and HD of the CN were performed, shown in Figs. 2 and 3. After obtaining the values of VD and HD, CSA of the nerve was calculated by using CSA=Ï(VD/2)(HD/2) formula.
Audiological examination
After middle ear pathologies were excluded by otologic examination and tympanometry test (AZ 26 Clinical Audiometer; Interacoustics, Assens, Denmark), pure tone audiometry test between 250 Hz and 8,000 Hz frequencies was performed in a soundproof cabin (AC 33 Clinical Audiometer, Interacoustics). Pure tone average (PTA) was calculated by arithmetic mean for frequencies of 250â8,000 Hz. The speech discrimination scores (SDS) were detected at an easily detectable hearing level by 50 selected monosyllabic words, and calculated by the percentage of words correctly identified. Pretreatment and posttreatment hearing levels were analyzed.
Upsloping (raising), downsloping (falling), U-shaped, and flat curves, and profound HL (hearing threshold shift higher than 90 dB in all frequencies) categories were used to classify the pretreatment audiograms.
The groups were also classified according to pretreatment PTA as follows: very severe (profound) (>90 dB), severe (71â90 dB), moderate to severe (56â70 dB), moderate (41â55 dB), mild (26â40 dB), and very mild (16â25 dB) HL.
Posttreatment recovery of PTA results was analyzed according to Furuhashi criteria (complete recovery: all 5 frequencies of final audiogram are 20 dB or less or improvement to the same degree of hearing as in the unaffected ear; marked improvement: PTA improvement >30 dB; slight improvement: 10 dB< PTA improvement <30 dB; no change: PTA improvement <10 dB) at the 6th month of treatment [9].
Treatment strategy
Methylprednisolone at a dose of 1 mg/kg/d was started orally and continued for about 10 days by reducing 16 mg every 3 days. If the patient was without complete recovery at the end of initial treatment, intratympanic steroid treatment (5 doses of 2 mg intratympanic dexamethasone once every 2 days) and hyperbaric oxygen therapy (2,5-atmosphere of 120 minutes for 20 consecutive days) were given respectively as salvage treatment.
Statistical analysis
IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA) was used for performing analysis of outputs. The Kolmogorov-Smirnov test was performed to test the normal distribution of data. The Mann-Whitney U test (for two groups) and the Kruskal-Wallis H or one-way analysis of variance tests (more than two groups) were used to compare groups. For categorical variables, chi-square test was performed. Statistical significance was defined as p<0.05.
The intraclass correlation coefficient (ICC) and the lower and upper limits of the 95% confidence interval were determined for intraobserver and interobserver variability and interpreted as follows: 0.0â0.2, poor correlation; 0.21â0.4, fair correlation; 0.41â0.6, moderate correlation; 0.61â0.8, good correlation; 0.81â1, almost perfect correlation.
Results
Participants
After 29 patients were excluded due to the before-mentioned reasons, 125 patients (59 [47.2%] women; mean age 47.7Âą13.8 years [minimumâmaximum: 21â76]) were included in this study.
The control group consist of 60 healthy participants (27 [45%] women; mean age 45.7Âą16.8 years [ranging from 20 to 76]). MRI examinations of 120 (right and left sides of 60 participants) sides were evaluated in the control group. There was no significant difference in gender and age between the study and the control group (p=0.76 and p=0.77, respectively).
Audiological test results
Pretreatment audiological test results (PTA and SDS) of control and study groups were shown in Table 1. Left ear was affected in 64 (51.2%) patients and the right ear was affected in 61 (48.8%) in the study group. Pretreatment audiogram types were flat in 36 (28.8%) patients, downsloping in 28 (22.4%) patients, upsloping in 26 (20.8%) patients, U-shaped in 18 (14.4%) patients, and profound in 17 (13.6%) patients. Pretreatment hearing levels were very mild in 8 (6.4%) patients, mild in 31 (24.8%) patients, moderate in 28 (22.4%) patients, moderate-severe in 29 (23.2%) patients, severe in 15 (12%) patients, and very severe in 14 (11.2%) patients.
Magnetic resonance image analysis results
The intraobserver and interobserver variability were small with the ICCs being 0.968 (0.907â0.989) and 0.959 (0.832â0.990), respectively. Measurements were then averaged for both readers. Magnetic resonance image analysis results in terms of HD, VD, and CSA of the CN were shown in Table 2.
The differences in CSA (0.10Âą0.17 mm2) and HD (0.05Âą0.15 mm) values between affected and unaffected sides in the study group were higher than the differences (CSA, 0.042Âą0.15 mm2; HD, 0.02Âą0.06 mm) between the affected side of the study group and control group (p=0.02 and p<0.012, respectively). Table 3 shows the age- and sex-adjusted general linear model analysis. According to this model, age and sex did not affect CN sizes. The values of VD, HD, and CSA did not differ between pretreatment audiograms types (p=0.23; p=0.53; p=0.39, respectively) and initial hearing levels (p=0.16; p=0.22; p=0.23, respectively).
Treatment response results
There were no differences in VD, HD, and CSA values between recovery groups according to Furuhashi criteria (p= 0.18; p=0.37; p=0.27, respectively). The treatment responses differ in groups of pretreatment audiogram types that were shown in Table 4. The treatment responses were also different according to initial hearing levels. Eight (100%) patients with very mild HL, 27 (87.1%) patients with mild HL, 14 (50%) patients with moderate HL, 9 (31%) patients with moderatesevere HL, 4 (3.2%) patients with severe HL, and 1 (7.1%) patient with very severe HL had complete recovery (p<0.001).
Discussion
Data from the current study show that patient with ISSHL had a smaller CSA of the CN, on the affected side, compared to the control group as well as on the unaffected side. Also, patient with ISSHL had a smaller VD and HD of the CN than control group. For the first time in the literature, the relationship between morphologic measurements of CN and the type of pretreatment audiograms was examined in the current study and it was found that the morphologic measurements of the CN did not have any relation with the type of pretreatment audiograms. Also, the morphologic measurements of the CN did not affect the treatment response; and the treatment responses of patients were only related to the type of pretreatment audiograms and the severity of pretreatment HL.
The 3D-CISS is a banding artifact-free type of gradient-echo MRI sequence. In this modality, image contrast is determined by the ratio of T2/T1. When structures are surrounded by cerebrospinal fluid, a perfect contrast between the cerebrospinal fluid and other structures is realized by 3D-CISS. Hence it is preferred in the imaging of the structures within the cerebellopontine angle and IAC. Another advantage is the applicability of this imaging method in MRI devices with 1.5-T as well as 3-T field strengths [10]. Nowadays, there are limited studies on CN morphologic measurements using 3D-CISS.
In a recent study, 53 patients with postlingual sudden HL for 5â20 years were evaluated by comparing the CN sizes with the healthy side ears. No difference was found between the CN sizes in the healthy and deaf sides of these patients. Mean values of HD and area of CN were determined as a mean of 0.82 mm and 1.16 mm in the healthy ear, 0.75 mm and 1.14 mm in the deaf side, respectively without statistically significant difference. This may be owing to small sample size of study and the absence of a control group [8].
Measurements of CN sizes by MRI technique have clinical significance in cochlear implant patients. In the study in which 68 postlingually sensorineural HL patients underwent cochlear implantation (CI) were included, there was a negative correlation between the prolongation of sensorineural HL and CSA. Although it was not statistically significant, a negative correlation was detected between the severity of HL and CSA. Also in this study, it was found that there was a positive correlation between CSA and hearing success after CI. The authors suggested that MRI could be used to foresee residual hearing and hearing success after CI in patients with postlingual sensorineural HL. Although this study provides important information between deafness and CN size, it does not fully reflect the CN size in ISSHL patients due to the heterogeneous group of the patients included in the study [7]. CN diameter was used in another study aiming to predict the results in cochlear implant patients [11].
In studies conducted on children with unilateral SSHL, CN size on the affected side was found to be smaller than that on the healthy side. This was found to be more pronounced, especially in patients with genetic disorders [12,13]. Nowadays, there are articles about the possibility of genetic disorders with ISSHL in adults, so there may be a high probability of differences between CN diameters in adults as shown in our study [14,15]. When the current literature is reviewed, it is considered that this condition is frequently related to late-onset genetic diseases in patients with bilateral profound sensorineural HL [16]. However, there is a need for further genetic studies showing that genetic predisposition also has an effect on unilateral SSNHL disease.
Apart from these studies using imaging methods, there are also morphological studies on the human temporal bone. In these cadaver studies, diameters of CNs were smaller in deaf subjects than those in normal controls [4]. In another cadaver study, a strongly positive correlation was found between the diameters of vestibulocochlear nerve (and also one by one cochlear and vestibular nerves), and residuary spiral ganglion cell count in patients with sensorineural HL [17]. These results may explain the fewer spiral ganglion cells found in patients with CNs of smaller diameters. In case of ischemia or inflammation, a scant amount of spiral ganglion cells present in ISSHL patients who have smaller CNs may be prone to loss of all these cells easily, whereas those patients with a sufficient amount of spiral ganglion cells may not lose all of these cells and be protected from ISSHL. This hypothesis may explain our findings in this study.
In our study, the main finding is the lower CN diameters in ISSHL patients. This may be a profound finding due to the fewer number of spiral ganglion cells in these patients as a result of several causes which can be congenital or acquired. As we have performed MRI imaging within 2 days of admission, we do not expect CN atrophy in such a short term, but an acute injury to spiral ganglion cells which are proposed to be profoundly lower in ISSHL by lower CN diameters is thought to be the main cause of SHL in our study population.
The definitive prognostic factors of ISSHL include advanced age, the severity of initial HL, existence of vertigo, concomitant comorbidities, and delay between starting theraphy and onset of symptoms [18-21]. In our study, in line with the literature, a relationship was found between curve type and recovery. It has been observed that patients with a U-shaped audiogram had the best prognosis. With regard to degree of HL, patients with severe HL had the worst prognosis. However, in our study, no relation was found between CN size and curve type, degree of HL, and response to treatment. This may support that the curve type and response to treatment were related to the affected area in the cochlea rather than the CN diameter.
Limitations of the study
The number of patients was relatively small to categorize according to the curve types, degrees of HL, and treatment response. This may be another reason why there is no relationship between audiogram curve types, pretreatment degree of HL, response to treatment, and CN diameter. Besides, prognostic factors of ISSHL could not be homogenized in terms of evaluation of response to treatment.
Conclusion
In our study, it has been shown that CN size may be a risk factor for ISSHL to occur. But CN size was not prognostic in terms of treatment response. These findings may explain why ISSHL disease is often unilateral; smaller diameter CN may indicate fewer spiral ganglion cells, indicating that the cochlea is more susceptible to ischemia or inflammation. Cohort studies involving larger numbers of participants are needed to support this hypothesis.