Introduction
More than 400 syndromes accompanied by deafness have been described, representing about 30% of cases of congenital deafness [1]. Among congenital deaf patients, 55% exhibited one or more disabilities like cognitive, behavioral, emotional, and motor disorders in addition to deafness.
While cochlear implantation (CI) in children typically leads to effective postoperative language development [2], a subgroup with inner ear anomalies, such as bony cochlear nerve canal narrowing, cochlear nerve hypoplasia or deficiency, and cochlear anomalies, showed less improvement in language development [3]. Children who have cognitive defects and several syndromes with disability also showed lesser improvement. Notably, the results of CI in children with complex needs were not always as sufficient or valuable as those without complex needs [4,5].
Children with additional needs were defined as those requiring additional support or interventions within the typical educational framework. Defining additional needs is difficult due to the wide range in severity, leading to a diverse group of children [6]. Also, children with additional needs have limitations in evaluating their language development because of the low neurodevelopment [7].
Social skills and adaptive behavior can be used to evaluate neurodevelopment. Social skills and adaptive behavior are measured using a Korean version of the Vineland Social Maturity Scale (VSMS) evaluated by clinical psychologists [8]. Using the results of VSMS, a social quotient (SQ) is calculated [9]. SQ is a rapid screening test for intelligence quotient and social adjustment [10,11]. Thus, this study aimed to evaluate the clinical characteristics and outcome of CI in children with additional needs and to compare their outcome with those of children without disabilities and from children with inner ear anomalies, matched for sex and age.
Subjects and Methods
Patients
The medical records of patients who received CI at a tertiary institution from January 2000 to December 2014 were retrospectively reviewed. They all underwent CI surgery prior to the age of 7 years. This retrospective study protocol was approved by the Institutional Review Board of Asan Medical Center (2018-1123). Taking informed consent was waived. Out of a total of 117 patients diagnosed with developmental delay and syndromes, 24 patients had an SQ of 70 or below. Evaluation of developmental delay was by a speech pathologists, pediatric clinical psychologists, and pediatricians.
VSMS test consists of 8 subscales: communication, general self-help ability, locomotion, occupation, self-direction, self-help eating, self-help dressing, and socialization. SQ of VSMS was calculated for adaptive behavior, with a standardized mean of 100 and a standard deviation of 15 [12]. We classified developmental delay into three subgroups based on the SQ; the groups into those with mild retardation for scores between 55 and 70, moderate retardation for scores between 40 and 54, and severe retardation for scores below 40.
To compare the postoperative results, two control groups were selected: normal control group and inner ear anomaly control group. The normal control group consisted of sexand age-matched 24 patients with normal development and SQ above 70. These children did not have inner ear anomaly. Children who received CI during the same period (2000–2014) were serially selected to be matched the sex and age. The inner ear anomaly control group comprised 38 children with typical development (SQ>70) and inner ear anomalies on preoperative imaging. Children in this group also received CI during the same period (2000–2014), but age and sex could not be matched. The mean SQ scores for each group were calculated to compare their outcomes after CI surgery.
Audiologic assessment and postoperative auditory performance
All children had bilateral severe to profound sensorineural hearing loss. Pure tone audiometry, auditory brainstem response, and auditory steady-state response were used for the hearing evaluation. Auditory performance was assessed using the Infant-Toddler Meaningful Auditory Integration Scale (IT-MAIS) and Categories of Auditory Performance (CAP) score. IT-MAIS and CAP tests were administered preoperatively and postoperatively, with a minimum follow-up period of 5 years.
IT-MAIS is designed for evaluating auditory abilities in infants and toddlers. The test consists of 10 questions, including three main areas: patients’ confidence in hearing devices (1–2 questions), auditory sensitiveness (3–6 questions), and ability to connect sounds with meaning (7–10 questions) [13]. Each question is answered with a range from 0 (never) to 4 (always) to indicate the frequency of the observed behavior. The total score ranges from 0 to 40 points. We record the IT-MAIS score as a percentage.
CAP scores can be evaluated into eight categories of increasing difficulty: 0=no awareness of environmental sound, 1=awareness of environmental sounds, 2=responds to speech sounds, 3=recognizes environmental sounds, 4=discriminates at least two speech sounds, 5=understands common phrases without lipreading, 6=understands conversation without lipreading with a familiar talker, and 7=can use the telephone with a familiar talker [14,15]. In order to compare auditory outcomes between patients with normal development children and those with developmental delay children, the scores of IT-MAIS and CAP were compared at 2 and 5 years postoperatively.
Statistical analysis
A descriptive analysis was used to show the clinical and demographic parameters. The Kruskal–Wallis test was used to compare the postoperative outcomes among patients with additional needs. In order to compare the results between each two groups, the independent t-test and Mann-Whitney test were used. A p-value of 0.05 or less was considered statistically significant. All statistical analysis and visualization were accomplished using either IBM SPSS Statistics version 22 (IBM Corp., Armonk, NY, USA) or GraphPad Prism version 9.1 (GraphPad Software Inc., San Diego, CA, USA).
Results
Demographics
Among the 24 patients diagnosed with developmental delays and having an SQ of 70 or below, the male-to-female proportion was 18/6 (75%/25%). The mean age at the time of surgery was 2.7±1.8 years old. The additional disabilities consisted of; CHARGE syndrome in 7 cases (29.2%); mental retardation in 4 (16.7%); cerebral palsy in 2 (8.3%); autism in 1 (4.2%); Down syndrome in 1 (4.2%); Dandy-Walker syndrome in 1 (4.2%), and developmental disorder without syndromes were 8 (33.3%) (Table 1). The mean SQ was 53.3: 14 (58.3%) with 55–70, 5 (20.8%) with 40–54, and 5 (20.8%) with <40.
Mean age at the time of surgery of children in normal control group was 2.7±1.8 years old. The mean SQ score of them was 106±15.5. Mean age at the time of surgery of children with inner ear anomaly control group was 2.5±1.5 years old. The mean SQ score of them was 99.8±21.8.
Outcomes
The average IT-MAIS score for 24 patients with additional needs and SQ<70 was 72.3 at the 2-year postoperative and 84.0 at the 5-year postoperative. Their average CAP score was 3.7 at the 2-year postoperative and 4.6 at the 5-year postoperative.
Table 2 shows the mean IT-MAIS and CAP scores measured at 2-year postoperative and 5-year postoperative according to the SQ. Preoperative SQ did not statistically correlate with the IT-MAIS and CAP scores at 2 and 5 years. However, the 2-year CAP scores showed remarkably close significance with preoperative SQ scores (p=0.055). The high SQ group (55–70) tended to show higher CAP scores than the low SQ group (40–54, below 40) at the 2-year postoperative follow-up.
Comparison with the control groups
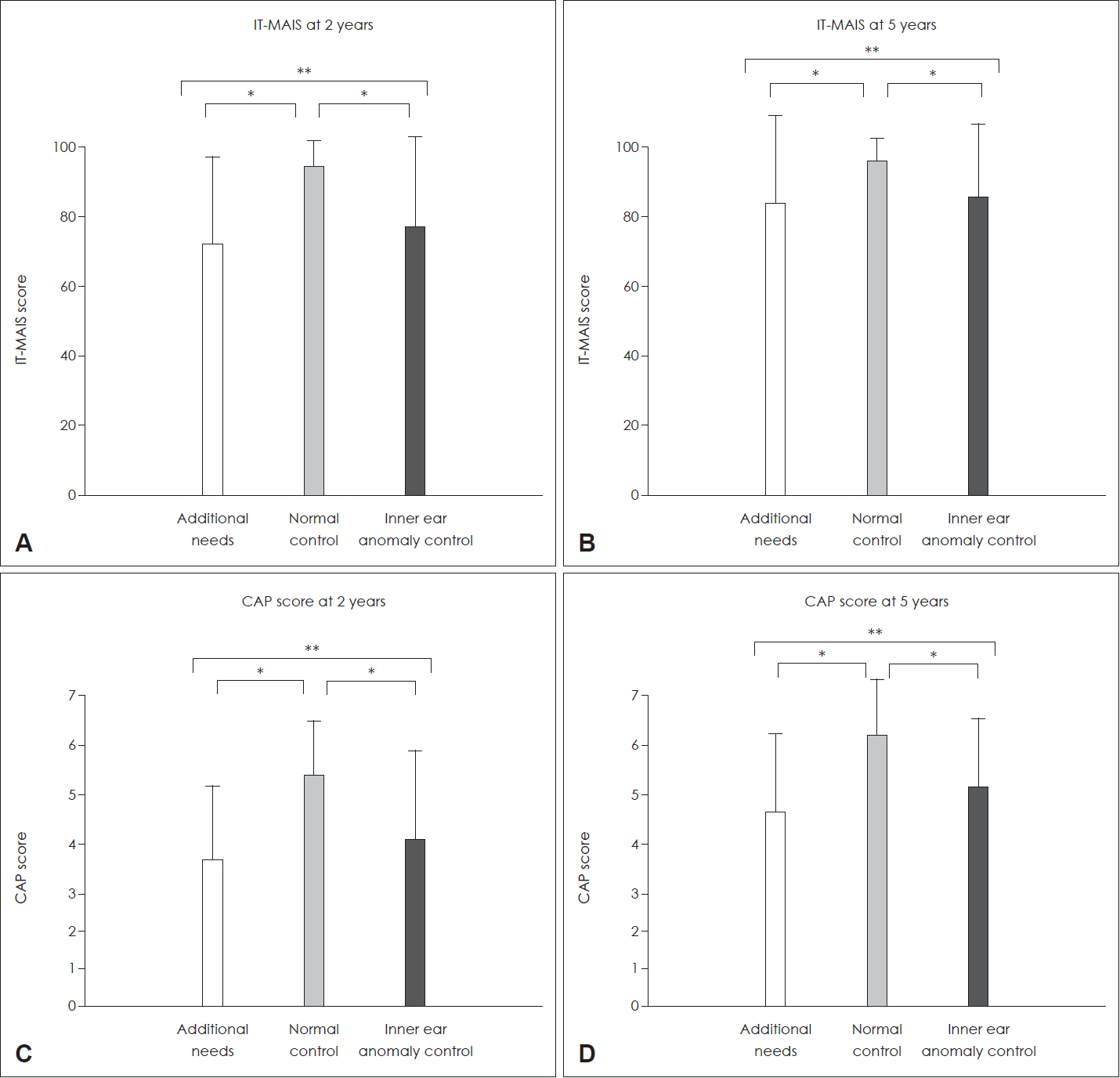
The sex- and age-matched control group was 24 patients. Their mean age at the time of surgery was 2.7 years old. The mean SQ was 106. The average IT-MAIS score for those patients was 94.4 at the 2 years and 96.3 at the 5 years postoperatively. The average CAP score at the 2 years was 5.4 and 6.2 at 5 years. There was a significant difference in IT-MAIS and CAP scores between children with additional needs and normal development at 2 and 5 years postoperative (Fig. 1)
The inner ear anomaly control group as a second control group consisted of 38 patients with inner ear anomalies. The mean SQ of them was 99.8. Their mean age at the time of surgery was 2.5 years old. The average IT-MAIS score was 77.2 at the 2 years and 85.7 at the 5 years postoperatively. The average CAP score at the 2 years was 4.1 and 5.1 at 5 years postoperatively.
Comparing the IT-MAIS among three groups at 2 years and 5 years after surgery, the normal development group showed better outcomes than the low SQ group (p<0.001, p=0.002, respectively) (Fig. 1). Also, it exhibited better outcomes than the inner ear anomaly group (p<0.001, p=0.004, respectively). However, there was no significant difference between the low SQ group and the inner ear anomaly control group at the 2 and 5 years after surgery in the IT-MAIS (p=0.467, p=0.754, respectively).
Comparing the CAP scores among three groups 2 and 5 years after surgery showed similar results. The normal control group showed better outcomes than the low SQ group (p<0.001, p<0.001, respectively) and also exhibited better outcomes than the inner ear anomaly control group (p=0.004, p=0.003, respectively). However, there was no significant difference between the developmental delay group and the inner ear anomaly group at 2 and 5 years after surgery in the CAP (p=0.325, p=0.194, respectively).
Inner ear anomalies within the developmental delay and syndrome children
Of 24 children with additional needs, 10 (41.7%) had inner ear anomalies. Among these, 7 (70%) had CHARGE syndrome, 1 (10%) had Down syndrome, and 2 (20%) had developmental delay only (Table 1).
Comparing the scores between children with inner ear anomaly (10 patients) and with normal structure (14 patients) did not show a significant difference in the average scores of IT-MAIS and CAP between the two groups in 2 and 5 years postoperative (Table 3).
Discussion
This study investigated the long-term auditory rehabilitation outcomes in children with additional needs and low SQ (<70) after CI surgery. Using the IT-MAIS and CAP scores, their results showed a gradual growth in auditor function over time. The patients achieved an average IT-MAIS score of 84.0 and an average CAP score of 4.6 at 5 years postoperative. Our findings showed that children with additional needs (developmental delays and syndromes) had variable outcomes on an individual but generally could benefit from CI surgery. It is consistent with previous studies reporting CI outcomes of developmental delay [4,16-18].
Our study showed the analysis of different syndrome categories, providing the influence of specific syndromes on CI outcomes. The presentation of CHARGE syndrome exhibits a diverse range of otologic manifestations, including external, middle, or inner ear abnormalities, sensorineural hearing loss, and facial palsy [19,20]. In our study, all patients with CHARGE syndrome exhibited inner ear anomalies. These patients initially exhibited lower IT-MAIS and CAP scores (72.7 and 4.0 at 2 years postoperative). However, these patients gradually improved, indicating the potential for auditory profit even in comorbidities (90.0 and 4.9 at 5 years postoperative).
There was one patient with autism in this study, and the maximum IT-MAIS score was 68, with the maximum CAP score being 2. Also, one patient with Down syndrome showed a SQ of 53. The maximum IT-MAIS score for this patient was 38, and the maximum CAP was 2.
A previous study showed that compliance with cochlear implants varies and seems to be associated with the severity of autism spectrum disorder [21,22]. Additionally, oral communication is unlikely to be a realistic goal for children with autism after CI, and traditional methods of evaluating the outcomes of CI in children with autism are often inadequate for a thorough assessment of the functional benefits [23]. Down syndrome is a genetic disorder caused by an anomaly in the 21st chromosome. Conductive hearing loss is observed in over 80% of children with Down syndrome [24,25]. Despite children with Down syndrome achieving a lower level of speech perception skills compared to non-syndromic peers, previous studies revealed that these individuals experienced satisfactory outcomes in terms of socialization, interest in the environment, and overall improvement in their quality of life [26,27].
Table 2 shows differences in CAP scores at the 2-year after CI surgery based on SQ. However, the results were similar at the 5-year follow-up. According to the results, it can be suggested that initial rehabilitation outcomes may be delayed in the low SQ group. However, after the 5-year, the results become comparable, indicating a potential delay in rehabilitation progress.
To investigate whether inner ear anomalies contribute to the CI outcomes beyond cognitive impairment, we evaluated the postoperative outcomes in children with additional needs with or without inner ear anomalies. Though inner ear anomalies can contribute to the postoperative results in children with SQ >70, there was no additional impact on the outcome in children with additional needs and SQ <70.
Cognitive impairment was the most critical factor in predicting CI outcomes [20,28,29]. Taken together, the postoperative results of CI in children with additional needs would be worse than the results in children with normal development. However, audiological rehabilitation with CI should be encouraged because there are audiologic benefits and improvement of social relationships. Therefore, if developmental delay is suspected or a syndrome is diagnosed before the CI surgery, conducting comprehensive evaluations, including preoperative SQ, genetic assessments, presence of inner ear anomalies, and other audiologic evaluations, would help predict CI outcomes accurately.
The limitation of this study is that we only used IT-MAIS and CAP scores to assess CI outcomes without considering functional activity. Due to their disabilities, language assessment is restricted, and the traditional method may have limitations in assessing patients [30]. Therefore, we must research comprehensive assessment methods during postoperative auditory rehabilitation.
In conclusion, CI outcomes in children with additional needs positively impacted auditory performance. While the postoperative auditory and language tend to improve slowly in children with additional needs and lower SQ, they gradually became more comparable to the other group of children over time. However, the improvement was less than that of the children without additional needs. Therefore, it is recommended to apply CI to children with additional needs, with long-term auditory rehabilitation following surgery.