Introduction
Middle ear adenoma, a very rare type of middle ear tumor, was first reported by Hyams and Michaels1) in 1976. Murphy, et al.,2) renamed it as carcinoid tumor which is similar to adenoma but is composed of neuroendocrine cells, and as seen on microscopic findings in 1980. Since then it has been called middle ear carcinoid tumor or middle ear adenoma.
In Korea, a total of three cases of adenomatous tumor in the middle ear have been reported. In 1978, Jun3) reported a case of adenomatous carcinoma, and in 1991 and 2000, Kwon, et al.4) and Jun, et al.5) reported respective cases of adenomatous tumor, but no subsequently reported case has been found through a literature review.
As middle ear tumors with glandular structure can differentiate to neuroendocrine cells and epithelial cells, middle ear carcinoid tumor and adenoma were initially classified as different tumors, although they are currently considered by the majority of researchers to be the same low-grade middle ear tumor.2) There is no clear definition regarding the derivation of the two tumors, although middle ear adenoma is divided into middle ear carcinoid tumor and middle ear adenoma.6)
We report a case of a 17-year old male patient who presented with repeated otorrhea and tinnitus in the left ear.
The patient underwent surgical treatment for middle ear polyps and was diagnosed with middle ear adenoma based on the postoperative pathology report.
Case Report
A 17-year old male presented with a two-year history of tinnitus and intermittent bloody otorrhea in the left ear. He had no definitive abnormal findings based on his past medical history. He had no accompanying symptoms such as otalgia, dizziness or facial paralysis.
The right tympanic membrane was normal. The left tympanic membrane was not perforated but was observed as having a milky-white, middle ear polyp which has approximately 3/4 of the eardrum protruded (Fig. 1).
Pure-tone audiometry showed normal hearing in the right ear and mixed hearing loss in the left ear with a 32-dB air-bone gap and a 37 dBHL air conduction threshold. Temporal bone CT findings showed a pneumatized mastoid cavity, although there was a soft tissue density which caused the eardrum to protrude outwardly, and filling of the inside of the mastoid antum, middle ear, and the epitympanum was observed. No structural damage of the ossicle, facial canal or lateral semicircular canal was identified (Fig. 2).
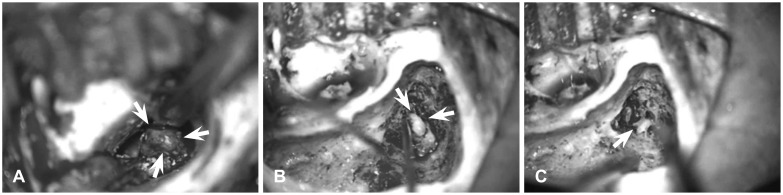
As left middle ear tumor or congenital cholesteatoma was suspected, we performed intact canal wall mastoidectomy with tympanization. According to the operative findings, a grayish-white multilobular mass and granulation tissue fully filling the mesotympanum, epitympanum, and mastoid cavity were detected (Fig. 3). The multilobular mass and granulation tissue were adjacent to the ossicle, although there was no ossicle erosion, and the hypotympanum and orifice of the Eustachian tube were preserved. No mass invasion into the sinus tympani was observed. Intact canal wall mastoidectomy was then performed, and the mass inside the epitympanium was excised by removing incus.
Tissue biopsy was performed to confirm the safety margin at the outer surface of the tympanic membrane which protruded to the external auditory canal because of the mass, mucosa of hypotympanum and epitympanum.
In these tissues, no tumor cells were observed. Ossiculoplasty to restore hearing was not performed. Rather, a temporalis muscle facial graft was performed.
Postoperative histopathologic results revealed a small, round-cell tumor composed of even-sized, globular cells with plenty of eosinophilic cytoplasm arranged in a platy structure. There were no findings of mitosis, necrosis or dysplastic were.
To obtain the differentiation diagnosis of small, round-cell tumor, immunohistochemistry was performed. Based on the findings which were negative to the Ki-67 antigen, positive to synaptophysin, mildly positive to CD56, negative to chromogranin, and negative to S-100 protein, middle ear adenoma was diagnosed (Fig. 4).
In the three weeks following surgery, all of the packing material in the external auricular canal was removed, and two months after the surgery, the eardrum was well-grafted and stabilized. Two and seven months after surgery, temporal bone CT and pure tone audiometry were both performed. Pure-tone audiometry showed 8 dBHL of the left bone conduction threshold and 32 dB of the air conduction threshold, both of which were similar to the patient's preoperative hearing level, however, the patient's tinnitus had improved. According to the temporal bone CT performed seven months after the surgery and otoscopy which was performed two years following the surgery, there was no evidence of recurrence.
Discussion
Since benign tumors of middle ear glandular tissue were reported by Hyams and Michaels1) in 1976, neuroendocrine tumor and middle ear adenoma have been separately described, but these tumors have been confused with ceruminoma, ceruminous adenocarcinoma, cystadenocarcinoma, ectopic salivary gland adenoma, adenocarcinoma, meningioma, and paraganglioma. Hypotheses such as the development of middle ear adenoma from the epithelial layer of the middle ear mucous gland1) and pluripotent endodermal stem cells located in the mucosa during the development of middle-ear-like pulmonary carcinoid tumor arising from Kulchitsky cells,7) have been suggested. Another study reported the similarity between the developing process of middle ear carcinoid tumor and those of adenoma, although the details regarding the orifin of middle ear neuroendocrine cells are still unknown. However, opinions opposed to the idea of a similarity between middle ear carcinoid tumor and middle ear adenoma, have been also proposed.8) And although it is still debatable, the opinions that middle ear adenoma can be differentiated from epithelial cells of mucous glands and neuroendocrine cells,9) and that tumors can develop from pluripotent basal cells10) or neural-crest-cell-derived glomus tissue,1) are widely supported these days. Accordingly, Saliba, et al.6) classified types of adenomas of the middle ear as neuroendocrine adenoma, middle ear adenoma, and middle ear carcinoid tumor in accordance with the immunohistochemistry and the presence of metastasis to other organs which is a known clinical feature of middle ear carcinoid tumor. According to the cases which have been reported up to now, the mean onset age of middle ear adenoma is 44.6 years of age (16-77 years) with a male to female ratio of 1.3 : 1 in favor of males, and there was no difference between the right and the left ears.6) In previous Korean reports, the patient ages were 39 and 43, and which were older than in our patient. The most common patient complaint was unilateral hearing impairment, with majority of patients showing conductive hearing loss. In some cases, symptoms of aural fullness, ear pain, otorrhea, tinnitus, dizziness, and facial paralysis were reported.3-5,7,12,13)
According to otoscopic findings, most of the cases showed a normal external auditory canal and eardrum. In the temporal bone CT findings, a soft tissue density surrounding ossicles and a relatively clear margin was observed.12) MRI was performed for patients who were suspected of having a malignant tumor. The MRI findings showed higher signal of tumor than the white matter in the T1 sequence, the same signal as the gray matter in the T2 sequence, and an enhancing mass in the gadolinium-enhanced T1 sequence.14)
In our patient, a protruded mass was observed on otoscopy and a soft tissue density filling epitympanum and mastoid cavity were observed on CT, although ossicle erosion was not observed. Therefore, MRI was not performed based on the assumption that the tumor was benign.
The differential diagnosis of middle ear adenoma includes inflammatory diseases such as cholesteatoma and chronic otitis media, and primary middle ear tumor such as ceruminoma, pleomorphic adenoma, paraganglioma, jugular body tumor, and metastatic cancer. For the differential diagnosis, immunohistochemistry is usually performed.
A 6-90% positive reaction to cytokeratin (such as CAM5.2, CK7 and CK20) which is an epithelial cell-derived probe, and a 15-88% positive reaction to chromogranin, neuron-specific enolase, synpatophysin, serotonin, human pancreatic polypeptide, and S-100 which is a neuroendocrine probe have been reported.15) With the present case, as findings of positive to synaptophysin and CK7, negative to chromogranin and S-100, and partially positive to cytokeratin and neuroendocrine probe were reported, the patient was diagnosed as having middle ear adenoma accompanying neuroendocrine differentiation.
In most cases, surgical treatments are performed using a transmastoid approach with tympanoplasty. In some cases, 45-60 Gy of post-operative radiation therapy is performed, although chemotherapy is not performed.6,12)
In previous reports, the recurrence rate was low but the time for developing recurrence ranged widely from 12 months to 43 years. In all recurrence cases the initial treatments were focused on the procedures used to preserve the ossicle surrounded by tumor and to remove the tumor only.6)
It is still controversial which is the most desirable treatment, although radical surgery such as complete removal of the tumor and ossicle, is considered to be able to reduce the recurrence rate. Considering the risk of developing a secondary cancerous tumor, the use of radiation therapy should also be given further consideration.6) The present case has been under observation for two years, during which no recurrence has been observed. However, considering the wide variety of recurrence times which have been reported in other studies, a long-term progress observation through routine physical exams and CT, is required.